Filter
1773
Text search:
Interval
Featured
190
484
Language
Document type
985
320
292
73
46
24
20
5
3
2
2
1
Countries
144
74
47
46
44
41
38
34
34
30
30
30
28
28
27
25
23
23
20
19
19
17
16
14
14
13
11
11
10
10
10
9
9
8
8
7
7
7
6
6
5
5
5
5
5
4
4
4
4
4
4
4
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
734
215
112
89
54
22
20
1
Toolboxes
158
136
130
75
60
57
46
44
35
32
31
29
29
26
23
21
14
13
13
11
11
9
9
4
2

This curriculum was designed to train newly recruited health care workers (HCW) in the basic knowledge and skills needed to improve different HIV services within the health facility including identification, linkage, retention and support. In addition to HIV basics, the training has supplementary un
...
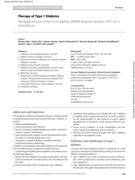
The document provides detailed clinical guidelines for the therapy of Type 1 Diabetes as developed by the German Diabetes Association (DDG). It focuses on individualized insulin therapy, structured patient training, and monitoring of blood glucose levels. The guidelines emphasize preventing complica
...

The document "Pocketbook for Management of Diabetes in Childhood and Adolescence in Under-Resourced Countries" (2nd Edition) provides practical guidelines for managing diabetes in children and adolescents, particularly in resource-limited settings. It covers key topics like diagnosing and treating d
...

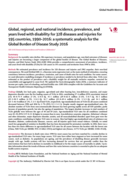
In recent decades, India has witnessed a rapidly exploding epidemic of diabetes.
Indeed, India today has the second largest number of people with diabetes in the
world. The International Diabetes Federation (IDF) estimates that there are 72.9 million people with diabetes in India in 2017, which is
...
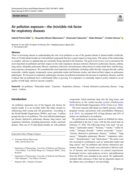
There is increasing interest in understanding the role of air pollution as one of the greatest threats to human health worldwide. Nine of 10 individuals breathe air with polluted compounds that have a great impact on lung tissue. The nature of the relationship is complex, and new or updated data are
...

The ICMR type 1 diabetes guidelines come at a time when the SARS-CoV-2 pandemic
has disproportionately affected people with diabetes population, exposing them to a
high risk for severe illness and mortality. Globally, diabetes was responsible for over fourmillion deaths in the year 2019. It was th
...

Smallpox eradication was certified in 1980. Mpox has been endemic in Central and West African countries since it was first detected in 1958 . It is a zoonosis; cases are often found close to tropical rainforests where various animals carry the orthopoxvirus that causes the disease. In endemic countr
...
The Global Status Report on Noncommunicable Diseases (NCDs) 2014 by the World Health Organization outlines the global impact of NCDs, including cardiovascular diseases, cancer, diabetes, and chronic respiratory diseases, which are responsible for a significant portion of global mortality, particular
...
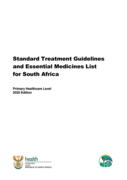
The "Primary Healthcare Standard Treatment Guidelines and Essential Medicines List" by the South African National Department of Health provides evidence-based guidelines for diagnosing and managing common medical conditions at the primary healthcare level. This document includes treatment protocols
...

Care for persons with noncommunicable diseases (NCDs), such as cardiovascular disease, diabetes, cancer, and chronic obstructive pulmonary disease, is a major health priority for most countries worldwide, particularly for low-middle income countries where the problem seems to be worsening. Globally,
...

This study compared clinical and autopsy findings for three asbestos-related diseases (asbestosis, mesothelioma and lung cancer) in former asbestos mineworkers, and explored factors that influenced agreement between clinical and autopsy findings using data from two compensation systems. In South Afr
...

Risk factors for asthma among schoolchildren who participated in a casecontrol study in urban Uganda
Data on asthma aetiology in Africa are scarce. We investigated the risk factors for asthma among schoolchildren (5–17 years) in urban Uganda. We conducted a case-control study, among 555 cases and 1115 controls. Asthma was diagnosed by study clinicians. The main risk factors for asthma were tertia
...

The epidemiology of wheeze in children, when assessed by questionnaires, is dependent on parents' understanding of the term “wheeze”.
In a questionnaire survey of a random population sample of 4,236 children aged 6–10 yrs, parents' definition of wheeze was assessed. Predictors of a correct
...

Over the past 20 years, the Global Initiative for Asthma (GINA) has regularly published and annually updated a global strategy for asthma management and prevention that has formed the basis for many national guidelines. However, uptake of existing guidelines is poor. A major revision of the GINA r
...

The 2023 update of the Global Strategy for Asthma Management and Prevention incorporates new scientific information about asthma based on a review of recent scientific literature by an international panel of experts on the GINA Science Committee. This comprehensive and practical resource about one o
...

The reader acknowledges that this report is intended as an evidence-based asthma management strategy, for the use of health professionals and policy-makers. It is based, to the best of our knowledge, on current best evidence and medical knowledge and practice at the date of publication. When assessi
...
Asthma is the most common chronic respiratory disease (CRD) worldwide and is estimated to affect 262 million causing significant mortality and morbidity, and has emerged as an important public health problem in many Latin American (LA) countries over the last 30 or so years. LA is a highly diverse r
...

Several challenges face asthma management in Egypt, including the high percentage of uncontrolled patients, inadequate compliance, and overuse of short-acting beta-agonists (SABAs) leading to increased asthma-related morbidity and mortality. In this regard, the recent Global Initiative for Asthma (G
...

Asthma is the most common noncommunicable disease in children, and among the most common in adults. According to the most recent estimates from the Global Asthma Network Phase I study, around one in 10 children and adults have symptoms of asthma and one in 20 school-aged children have severe asthma
...

The pharmacological management of asthma has changed considerably in recent decades, as it has come to be understood that it is a complex, heterogeneous disease with different phenotypes and endotypes. It is now clear that the goal of asthma treatment should be to achieve and maintain control of the
...