Filter
4367
Filtered Results: 4367
Text search:
PC
Featured
Recommendations
465
New Publications
1050
Language
Document type
No document type
2030
Guidelines
868
Studies & Reports
700
Manuals
215
Strategic & Response Plan
188
Fact sheets
155
Training Material
74
Situation Updates
51
Infographics
30
Brochures
19
Resource Platforms
19
Online Courses
10
Videos
4
Dashboards/Maps
3
App
1
Countries / Regions
India
180
Congo, Democratic Republic of
145
Global
129
Brazil
118
Senegal
90
Africa
90
Kenya
87
Germany
85
Nigeria
79
South Africa
78
Latin America and the Carribbean
77
Western and Central Europe
69
Ethiopia
63
Rwanda
61
Burkina Faso
58
Liberia
58
Nepal
57
Mozambique
57
Uganda
55
Sierra Leone
51
Tanzania
50
Benin
49
Zambia
42
Colombia
39
Malawi
39
Peru
38
Myanmar / Burma
38
Haiti
37
Bangladesh
37
Guinea
36
Paraguay
36
Syria
35
West and Central Africa
34
Argentina
34
Philippines
33
Middle East and North Africa
33
Russia
32
Indonesia
32
Cameroon
31
Madagascar
31
Ghana
30
Venezuela
28
Bolivia
28
Angola
28
East and Southern Africa
25
Central African Republic
25
Mali
25
Ecuador
25
Ukraine
24
Chile
23
Zimbabwe
22
Eastern Europe
22
Namibia
22
El Salvador
21
Yemen
20
Lesotho
17
South Sudan
17
Côte d’Ivoire / Ivory Coast
15
Cambodia
14
Spain
14
South–East Asia Region
12
Eastern Europe and Central Asia
12
Botswana
12
Togo
11
Niger
11
Chad
11
Pakistan
11
Guinea-Bissau
10
Sudan
9
Eswatini/ Swaziland
9
Asia
8
France
8
Somalia
8
Mexico
7
Afghanistan
7
Burundi
7
Italy
7
Guatemala
7
Thailand
6
China
6
Lebanon
6
Vietnam
6
Honduras
6
Iraq
6
Laos
5
Congo-Brazzaville
5
USA
5
Jordan
5
Portugal
5
Sri Lanka
5
Turkey
4
Dominican Republic
4
Saudi Arabia
4
Western Pacific Region
4
Uruguay
4
Papua New Guinea
4
Palestine
4
Iran
3
Albania
3
Canada
3
Morocco
3
North America
3
Nicaragua
3
Moldova
3
Libya
3
North Macedonia
2
Switzerland
2
Timor Leste/ East Timor
2
Qatar
2
Mauritania
2
Mauritius
2
Southern Africa
2
Djibouti
2
Serbia
1
Australia
1
Gambia
1
Kazakhstan
1
Estonia
1
Uzbekistan
1
Austria
1
Bulgaria
1
Armenia
1
Hungary
1
Luxembourg
1
Denmark
1
Belgium
1
Maldives
1
Tunisia
1
United Kingdom
1
Egypt
1
Romania
1
Slovakia
1
Georgia
1
Poland
1
Cuba
1
Authors & Publishers
Publication Years
Category
Countries
2018
Clinical Guidelines
380
Public Health
152
Women & Child Health
147
Key Resources
138
Pharmacy & Technologies
75
Capacity Building
69
Toolboxes
COVID-19
739
TB
252
NTDs
243
HIV
189
Ebola & Marburg
186
Mental Health
161
Rapid Response
129
AMR
121
Caregiver
109
Planetary Health
100
Zika
87
Global Health Education
78
Malaria
73
NCDs
62
Pharmacy
61
Refugee
58
Disability
54
2.0 Rapid Response
49
Conflict
46
Cholera
34
Health Financing Toolbox
23
Polio
21
Natural Hazards
16
Specific Hazards
15
Social Ethics
15
Typhoon
2

J Fungi (Basel) . 2019 Aug 16;5(3):75. doi: 10.3390/jof5030075 . Namibia is a sub-Saharan country with one of the highest HIV infection rates in the world. Although care and support services are available that cater for opportunistic infections related to HIV, the main focus is narrow and predominan...


Mars 2020. Recommendations selon les differentes phases


Indonesia's TB Guidelines

Ce profil pays est le résultat d'une évaluation du paysage menée par le personnel et les collègues d'Advancing Partners & Communuties (APC). Cette évaluation du paysage portait sur les pays prioritaires de l'Agence des États-Unis pour le Développement International (USAID) en termes de Popula...

6th edition. The HIV epidemic Namibia is gradually being brouhgt under countrol as demonstrated by results in the preliminary report of Namibia Population-Based HIV Impact Assessment (NAMPHIA), a cross-sectional household-based survey that was conducted in 2017. Currently, it is estimated that about...

Sudan virus disease is a severe, often fatal illness affecting humans and other primates that is due to Orthoebolavirus sudanense (Sudan virus), a viral species belonging to the same genus of the virus causing Ebola virus disease. This webinar will provide an overview of the current outbreak of Suda...

Accessed on 20.08.2022#
Actualización en Profilaxis Post Exposición (PPE) en Niños, Niñas y Adolescentes

National Guidelines for Antiretroviral Therapy
recommended

The Councils share a common mandate of ensuring persons practising health related professions in Namibia are suitably qualified. Registration with the Councils is, thus, a pre-requisite for professional practice – and it is also a legal requirement too update personal details of all registered hea...

The Healthy Living Toolkit is developed to educate refugees, immigrants, resettlement agencies, clinics, community based organizations, and other service providers on refugee health issues. The toolkit presents material in a culturally appropriate manner and is intended to help health care-related p...

Quem deve usar este documento
Esta lista de verificação destina-se a supervisores que apoiam os encarregados de realizar a vacinação contra a COVID-19.
Quando usar este documento
Use este documento para se preparar e conduzir
visitas de supervisão, presenciais ou remotas.


What measures can we take to overcome the corona crisis, limit its consequences or use scarce resources efficiently? Every day we experience uncertainties and contradictions on these questions among scientists, health experts, politicians and in society. We must all strive for a broad consensus to o...
(Published with Decision No. 3003/QðBYT dated 19/8/2009 of the Minister of Health)

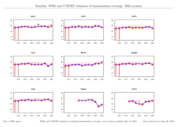
Each year WHO and UNICEF jointly review reports submitted by Member States regarding national immunization coverage, finalized survey reports as well as data from the published and grey literature. Based on these data, with due consideration to potential biases and the views of local experts, WHO an...
WHO guidelines on meningitis diagnosis, treatment and care. Web Annex A. Quantitative evidence reports
recommended
The guidelines are primarily intended for health-care professionals working in first- or second-level health-care facilities, including emergency, inpatient and outpatient services. They are also directed at policy-makers, health-care planners and programme managers, academic institutions, non-gover...