Filter
276
Filtered Results: 276
Text search:
maladies
cardiovasculaires
Featured
Recommendations
28
New Publications
57
Language
Document type
No document type
114
Guidelines
57
Studies & Reports
53
Strategic & Response Plan
14
Fact sheets
13
Manuals
12
Infographics
5
Training Material
3
Situation Updates
3
Brochures
1
Resource Platforms
1
Countries / Regions
Senegal
20
Benin
15
Global
15
Congo, Democratic Republic of
14
Burkina Faso
12
Haiti
8
Latin America and the Carribbean
8
Togo
6
Cameroon
6
Central African Republic
5
Niger
4
Africa
4
Luxembourg
4
Mali
4
West and Central Africa
3
East and Southern Africa
3
Madagascar
3
Burundi
2
Middle East and North Africa
2
Western and Central Europe
2
France
2
Bolivia
2
Brazil
2
Colombia
1
Rwanda
1
Canada
1
Congo-Brazzaville
1
Guinea
1
Germany
1
Belgium
1
Côte d’Ivoire / Ivory Coast
1
South Africa
1
Eastern Europe
1
Djibouti
1
Chad
1
Ecuador
1
India
1
Bahamas
1
Authors & Publishers
Publication Years
Category
Countries
102
Clinical Guidelines
68
Public Health
27
Women & Child Health
6
Key Resources
5
Capacity Building
2
Pharmacy & Technologies
2
Toolboxes
NCDs
35
COVID-19
34
Mental Health
21
Caregiver
13
Planetary Health
9
NTDs
7
Disability
5
HIV
4
TB
4
Malaria
4
Rapid Response
3
Refugee
2
Pharmacy
2
Global Health Education
2
Natural Hazards
1
Cholera
1
Ebola & Marburg
1
Conflict
1

The South African (SA) guidelines for cardiac patients for non-cardiac surgery were developed to address the need for cardiac risk assessment and risk stratification for elective non-cardiac surgical patients in SA, and more broadly in Africa.
The guidelines were developed by updating the Canadian ...

Lancet 2012; 380: 611–19
Series: Hypertension 3
Prevention of Cardiovascular Disease. Pocket Guidelines for Assessment and Management of Cardiovascular Risk
recommended
These pocket guidelines provide evidence-based guidance on how to reduce the incidence of first and recurrent clinical events due to coronary heart disease (CHD), cerebrovascular disease (CeVD) and peripheral vascular disease in two categories of people
Primary care health centers and providers who care for individuals with hypertension and cardiovascular disease have an important role to play in ensuring continued access to care, reducing the risk of coronavirus infection, and appropriately managing people with these co-morbidities who acquire COV...
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV‑2) causing coronavirus disease 2019 (COVID-19) has reached pandemic levels;
Patients with cardiovascular (CV) risk factors and established cardiovascular disease (CVD) represent a vulnerable population when suffering from COVID-19;
Patien...
Myocardial infarctions are generally clinically classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI), based on changes in ECG. When blood flow to a part of the heart stops or the heart is injured and fails to receive enough oxygen required for its adequate functioning the conditi...

Technical package for cardiovascular disease management in primary health care.

The World Heart Federation (WHF) has been advocating globally for stronger
legislation and policy regarding cardiovascular disease (CVD) for many years. Now, as focus shifts from global to national progress, we call on members and colleagues to advocate for greater action on CVD in your local setti...
Cardiovascular disease (CVD) is the leading cause of death in the Americas and raised blood pressure accounts for over 50% of CVD. In the Americas over a quarter of adult women and four in ten adult men have hypertension and the diagnosis, treatment and control are suboptimal. In 2021, the World Hea...
second edition
Included more self-measured blood pressure (SMBP)-focused content with tools and resources.
Showcased more tools to find patients with potentially undiagnosed HTN.
Added new strategies that focus on chronic kidney disease testing and identification.

Many low-resource settings have a shortage of physicians and health workers. (1) In order to provide patient-centred continuous care more effectively, primary care systems can include team-based care strategies in their clinic workflows and protocols. Team-based care uses multidisciplinary teams (wh...

Global Hear, March 2014, Vol. 9 no.1




This technical package provides a strategic approach to improving cardiovascular health in countries. It comprises six modules and an implementation guide. This package supports Ministries of Health to strengthen CVD management in primary health care settings. The practical, step-by step modules are...

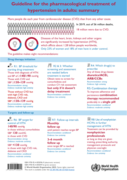
This report compiles data for the first time on the far-reaching consequences of uncontrolled hypertension, including heart attacks, strokes and premature death, along with substantial economic losses for communities and countries. It also contains information on the global, regional and country-lev...

The American Heart Association and the American College of Cardiology are excited to provide a series of cardiovascular prevention guidelines for the assessment of cardiovascular risk, lifestyle modifications that reduce risk, management of elevated blood cholesterol, and management of increased bod...