Filter
9240
Text search:
country
level
Featured
804
2528
Language
9011
206
165
117
84
62
41
30
11
10
10
9
8
7
7
7
6
6
6
6
5
5
5
5
5
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
Document type
4789
1864
1128
544
404
184
162
89
30
21
11
4
3
1
Countries
468
423
268
217
210
206
190
187
180
176
175
170
151
148
147
134
131
126
124
124
120
102
87
81
75
66
65
64
64
63
62
61
59
59
58
55
50
47
47
44
43
42
41
40
38
37
35
34
30
30
29
29
24
22
21
21
20
20
19
19
19
16
16
15
14
14
14
14
14
13
12
12
11
11
11
11
9
9
9
9
8
8
8
8
7
7
7
7
7
7
6
6
6
6
6
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
1307
397
323
262
235
197
158
131
93
92
90
57
51
50
46
45
44
42
40
37
35
34
32
32
31
30
30
30
29
29
28
28
27
27
27
27
26
26
25
24
24
23
23
22
22
22
21
21
21
21
21
21
20
20
20
20
20
18
18
18
18
18
18
18
17
17
17
17
16
16
16
16
16
16
16
16
15
15
15
15
15
15
14
14
14
14
14
14
13
13
13
13
13
12
12
12
12
12
12
12
12
12
12
12
12
12
11
11
11
11
11
11
11
10
10
10
10
10
10
10
10
10
10
10
10
10
9
9
9
9
9
9
9
9
9
9
9
9
9
9
9
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Publication Years
1
2939
5502
751
44
2
1
Category
3716
625
573
507
501
177
91
1
Toolboxes
738
645
420
412
373
308
281
278
265
248
236
194
190
178
176
172
155
142
131
128
62
57
50
40
34
7
2

This report aims to support countries in the necessary transition toward healthier, more sustainable diets by integrating biodiversity in food-based interventions to support nutrition and health. It is intended to help guide decision-makers in the health, nutrition and other sectors, to:
Consider
...
the important role of biodiversity in food systems for the development of integrated interventions to support healthy, diverse and sustainable diets;
To focus investments and country support for more comprehensive, coordinated and cross-cutting public health and nutrition projects and policies; and
To strengthen the resilience of food systems, health systems, and societies, each of which are each increasingly compromised by widespread ecological degradation, biodiversity loss and climate change.
Biodiversity at every level (genetic, species and ecosystem level) is a foundational pillar for food security, nutrition, and dietary quality. It is the basic source of variety in essential foods, nutrients, vitamins and minerals, and medicines, and underpins life-sustaining ecosystem services. It is a core environmental determinant of health, often a vital ingredient of healthy nutritional outcomes and livelihoods, gender equality, social equity, and other health determinants.
Biodiversity can play a more prominent role in planning for nutritional outcomes in various ways, e.g. by facilitating the production of nutritious fruits and plant products, sustaining livelihoods through more efficient production and increasing the diversity of products available in markets. This Guidance presents and expands on six core building blocks for mainstreaming biodiversity for nutrition and health:
Cross-sectoral knowledge development and knowledge co-production;
Enabling environments;
Integration;
Conservation and the wider use of biodiversity;
Education and awareness-raising;
Monitoring and evaluation;
This WHO report builds on an unprecedented opportunity to mainstream biodiversity in order to support healthy and sustainable diets, and offers the necessary technical guidance to catalyze and support a transformation of the global food system and transition to healthier, more sustainable diets.
more

3rd edition. In 2001, Uganda adapted the Integrated Disease Surveillance and Response (IDSR) developed by World Health Organization (WHO) for member states in African region. The Ministry of Health has been implementing the IDSR strategy since then with success across the
...
country. This strategy provides the opportunity for rational use of resources and maximises investments in health surveillance systems. The 3rd edition IDSR guidelines incorporates lessons learnt from previous
epidemics, new frameworks like the Global Health Security Agenda (GHSA), One Health, Disaster Risk Management (DRM), the WHO regional strategy for health security and emergencies, and the rising non-communicable diseases, and aims to strengthen implementation of IHR (2005) core surveillance and response capacities. These guidelines have been adapted to reflect national priorities, policies and public health structures; and shall be used in conjunction with other similar
guidelines/strategies or initiatives.
Overall, the 3rd edition technical guidelines will incorporate the following:
• Strengthening Indicator Based Surveillance
• Strengthening Event Based Surveillance
• Improving community-based disease surveillance
• Improving Cross Border Surveillance and response
• Scaling up e-IDSR implementation
• Improving reporting and information sharing platforms
• Improved data sharing across sectors
• Tailoring IDSR to Emergency or Disaster contexts
The 3rd edition guidelines are intended for use as:
• A general reference for surveillance activities across all levels
• A set of definitions for thresholds that trigger some action for response
• A stand-alone reference for level-specific guidelines on surveillance and response
• A resource for developing training, supervision and evaluation of surveillance activities
• A guide for improving early detection and preparedness for outbreak response.
more

Int. J. Environ. Res. Public Health 2022, 19, 9313. https://doi.org/10.3390/ijerph19159313. A mixed-methods study, using an online survey and in-depth interviews, was conducted. Participants included Mental Health Focal Points at the Ministries of Health, the World Health Organization (WHO)
...
country and regional offices, and civil society representatives. Responses were received from 28 countries out of 55 contacted. The implementation level, based on standard guidelines, of MHPSS activities was below 50% in most countries. The most implemented MHPSS activities were establishing coordination groups (57%) and developing MHPSS strategy (45%), while the least implemented activities included implementing the developed MHPSS strategy (32%) and establishing monitoring and evaluation mechanisms (21%). Key factors that hindered implementing MHPSS activities included lack of political commitment and low prioritisation of mental health during emergencies, as it was seen as a “less important” issue during the COVID-19 pandemic, when more importance was given to infection prevention and control (IPC)
more

Hand hygiene is vital for safe health care delivery, yet practices at the point of care remain suboptimal worldwide. A comprehensive research agenda is therefore necessary to improve our understanding of factors influencing hand hygiene behaviour and to strengthen appropriate interventions. This age
...
nda will provide insightful ideas for researchers to focus their projects and funding proposals and will direct donors towards the areas of hand hygiene evidence that require urgent support and innovation. It will also guide decision-makers and stakeholders at the national and international level and support country efforts in updating and strengthening hand hygiene promotion programmes. Global collaboration and investment in hand hygiene research remain essential to promote safe and effective care worldwide.
more
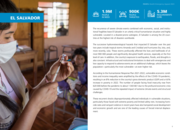
The recurrence of severe climate events combined with economic, social, and institutional fragilities leave El Salvador in an utterly critical humanitarian situation and highly vulnerable. Located in a disaster-prone subregion, El Salvador is among the 20 countries at the highest risk of disasters w
...
orldwide. The successive hydrometeorological hazards that impacted El Salvador over the past two years include tropical storms Amanda and Cristóbal and hurricanes Eta, Iota, and,
more recently, Julia. These storms profoundly affected the lives and livelihoods of almost 900 000 people and significantly disrupted health services, especially at the first level of care. In addition, the country’s exposure to earthquakes, floods, and droughts is also constant. Infrastructural and institutional limitations to deal with emergencies and
low capacity to respond to adverse events are an additional challenge, which leaves the population—particularly the most vulnerable—at even higher risk.
more

The overall objective of the framework is to support WHO and Members States in meaningful engagement of people living with NCDs, and mental health and neurological conditions to co-create and enhance related policies, programmes and services. This framework will contribute to advancing understanding
...
, knowledge and action on meaningful engagement and related participatory approaches from an evolving evidence base. It provides practical guidance and actions for transitioning from intention to action to operationalize meaningful engagement.
The aim of the framework is to guide people working at WHO and in Member States in ensuring meaningful engagement with individuals with lived experience. WHO will advocate for, provide technical assistance and operationalize implementation at its three levels (headquarters, regional and country offices) and will support Member States in implementation at national level through established processes and procedures.
more
The Generic All-Hazards Risk Assessment and Planning Tool for Mass Gathering Events (“All-Hazards MG RA Tool”) aims to support Member States and mass gathering events organizers.
The tool is based on the principles of the World Health Organization’s Strategic Toolkit for Assessing Risk (STA
...
R) as well as lessons learned identified from the COVID-19 Risk Assessment Tool for Mass Gatherings. The purpose of the All-Hazards Mass Gatherings Risk Assessment tool is to identify hazards related to the event, assess and quantify the overall level of risk, identify and account for precautionary measures that may reduce the risk, making the event safer. The tool provides a systematic evidence-based approach to identifying and classifying priority risks; a description of the level of national preparedness and readiness to mitigate specific hazards; guidance on the implementation of a comprehensive and strategic risk assessment to inform preparedness and response plans ahead of the mass gathering; and an estimated assessment of the host country capacity to identify and respond to potential negative health impacts.
more
To assess the impact of the COVID-19 pandemic on health and HIV expenditure, UNAIDS carried out a modelling study on fiscal space for health and HIV. From a sample of 28 countries, three countries—the Democratic Republic of the Congo, Jamaica, and Lesotho—were selected to capture health and HIV
...
expenditure impacts across countries with especially marked differences in burdens of disease (including HIV prevalence), HIV donor dependency, level of economic development, and geographic location. While the three-country sample is too small to permit findings to be generalized to other countries, these analyses are useful for informing UNAIDS’ work to identify some policy positions to minimize the COVID-19 pandemic’s impact on the HIV response.
more

This report describes the “Building health workers capacity on air pollution and health” pilot workshop held in Ghana in 2022 which aimed at testing the training material of the first WHO Air Pollution and Health Training toolkit (APHT) targeting health professionals. APHT aims at strengthening
...
the knowledge of health workers on air pollution and health and to enable them to effectively communicate with patients and communities on how to reduce their risk, to advocate for population level interventions as well as to train other peers and colleagues using a train-the-trainer approach. This workshop report serves as a tool and example of a training that can be replicated and adapted to other contexts and settings based on country and regional priorities and needs.
more

Introduction
In 2017, development assistance for health (DAH) comprised 5.3% of total health spending in lowincome countries. Despite the key role DAH plays in global health-spending, little is known about the characteristics of assistance that may be associated with committed assistance that is a
...
ctually disbursed. In this analysis, we examine associations between these characteristics and disbursement of committed assistance.
Methods
We extracted data from the Creditor Reporting System of the Organization for Economic Co-operation and Development, Institute for Health Metrics and Evaluation, and the WHO National Health Accounts database. Factors examined were off-budget assistance, administrative assistance, publicly sourced assistance and assistance to health systems strengthening. Recipient-country characteristics examined were perceived level of corruption, civil fragility and gross domestic product per capita (GDPpc). We used linear regression methods for panel of data to assess the proportion of committed aid that was disbursed for a given country-year, for each data source.
Results
Factors that were associated with a higher disbursement rates include off-budget aid (p<0.001), lower administrative expenses (p<0.01), lower perceived corruption in recipient country (p<0.001), lower fragility in recipient country (p<0.05) and higher GDPpc (p<0.05).
Conclusion
Substantial gaps remain between commitments and disbursements. Characteristics of assistance (administrative, publicly sourced) and indicators of government transparency and fragility are also important drivers associated with disbursement of DAH. There remains a continued need for better aid flow reporting standards and clarity around aid types for better measurement of DAH.
more

Ethiopia has been repeatedly affected by conflict, flooding, drought, and disease outbreaks in the past years. As of January 2024, the country is actively responding to the longest recorded cholera outbreak which started in August 2022, recurrent me
...
asles outbreaks which started in August 2021, and the highest number of malaria cases reported since 2017. The El Niño phenomenon is expected to cause further havoc up to July 2024, by causing drought in some parts of the country, and flooding in others. Food insecurity due to lost harvest and livestock is aggravating already high malnutrition rates, negatively impacting morbidity and mortality.
The Health Cluster is closely collaborating with the Ministry of Health (MOH) to prepare for, prevent, and respond to public health emergencies by mobilizing resources to enable health partners to provide life-saving health services to vulnerable populations.
In an environment with ever-increasing needs and decreased funding, the below priorities for 2024 and 2025 have been identified: 1 Strengthen advocacy for longer-term, development funding to address root causes of recurrent disease outbreaks, including through the Humanitarian-Development-Peace Nexus 2 Advocate for increased access to quality health services, with a strong focus on:
sexual and reproductive health services (including for survivors of sexual and gender-based violence)
inclusion of people with disabilities, older people, and people living with HIV
remote populations through inclusion of Mobile Health Teams (MHT) as part of the health system 3 Standardize health services provided by Health Cluster partners through the implementation of Essential Health Care packages, aligned with existing MOH guidance, aimed at ensuring quality service delivery for affected populations, especially at community level 4 Strengthen quality of, and access to data for needs analysis and informed decision-making 5 Strengthen subnational coordination, with increased focus on zones and local health partners
more
The Global Aids Strategy 2026-2031
recommended
United- Towards Ending AIDS. The Global AIDS Strategy 2026-2031 focuses global efforts for the future of the AIDS response to end AIDS as a public health threat by 2030 and sustain the HIV response after 2030. This is a strategy uniting the world.
The Strategy will shape the June 2026 United Natio
...
ns General Assembly High-Level Meeting on Ending AIDS and its political declaration. It provides all actors in the field with guidance to overcome the challenges and to ensure effective country-led AIDS responses. The Global AIDS Strategy 2026-2031 includes new global targets for 2030 and resource needs estimates.
more
United- Towards Ending AIDS. The Global AIDS Strategy 2026-2031 focuses global efforts for the future of the AIDS response to end AIDS as a public health threat by 2030 and sustain the HIV response after 2030. This is a strategy uniting the world.
The Strategy will shape the June 2026 United Natio
...
ns General Assembly High-Level Meeting on Ending AIDS and its political declaration. It provides all actors in the field with guidance to overcome the challenges and to ensure effective country-led AIDS responses. The Global AIDS Strategy 2026-2031 includes new global targets for 2030 and resource needs estimates.
more

Monitoring is a crucial element in any successful programme. It is important to
know if health care facilities – and ultimately countries – are meeting the agreed
goals and objectives for preventing and managing cardiovascular diseases (CVD).
Monitoring is the on-going collection, management
...
and use of information to
assess whether an activity or programme is proceeding according to plan and/
or achieving defined targets. Not all outcomes of interest can be monitored. Clear
outcomes must be identified that relate to the most important changes expected to result from the project and to what is realistic and measurable within the timescale of the project. Once these outcomes have been articulated, indicators can be chosen that best measure whether the desired outcomes are being met.
To allow progress to be monitored, this module provides a set of indicators on
CVD management. Agreeing on a set of indicators allows countries to compare
progress in CVD management and treatment across different districts or
subnational jurisdictions, as well as at a facility level, identify where performance
can be improved, and track trends in implementation over time. Monitoring
these indicators also helps identify problems that may be encountered so that
implementation efforts can be redirected.
This module starts from the collection of data at facility level, which is then
“transferred up” the system: facility-level data are aggregated at subnational level
to produce reports that allow tracking of facility and subnational performance over time and allow for comparison among facilities. National-level data are obtained through population-based surveys.
Implementing a monitoring system requires action at many levels. At national and
subnational levels, staff can determine how best to integrate data elements into
existing data collection systems – such as the routine service-delivery data that are collected through facility-level Health Management Information Systems (HMIS).
In the facility setting, personnel must be aware of what data are needed. Sample
data-collection tools are included, recognizing that countries use different datamanagement systems for HMIS, so the CVD monitoring tools will be adapted to work with the HMIS system being used by the country, such that the indicators can be collected with minimal disruption/work to existing systems and tools
more

To guide One Health capacity building efforts in the Republic of Guinea in the wake of the 2014–2016 Ebola virus disease (EVD) outbreak, we sought to identify and assess the existing systems and structures for zoonotic disease detection and control. We partnered with the government ministries resp
...
onsible for human, animal, and environmental health to identify a list of zoonotic diseases – rabies, anthrax, brucellosis, viral hemorrhagic fevers, trypanosomiasis and highly pathogenic avian influenza – as the country's top priorities. We used each priority disease as a case study to identify existing processes for prevention, surveillance, diagnosis, laboratory confirmation, reporting and response across the three ministries. Results were used to produce disease-specific systems “maps” emphasizing linkages across the systems, as well as opportunities for improvement. We identified brucellosis as a particularly neglected condition. Past efforts to build avian influenza capabilities, which had degraded substantially in less than a decade, highlighted the challenge of sustainability. We observed a keen interest across sectors to reinvigorate national rabies control, and given the regional and global support for One Health approaches to rabies elimination, rabies could serve as an ideal disease to test incipient One Health coordination mechanisms and procedures. Overall, we identified five major categories of gaps and challenges: (1) Coordination; (2) Training; (3) Infrastructure; (4) Public Awareness; and (5) Research. We developed and prioritized recommendations to address the gaps, estimated the level of resource investment needed, and estimated a timeline for implementation. These prioritized recommendations can be used by the Government of Guinea to plan strategically for future One Health efforts, ideally under the auspices of the national One Health Platform. This work demonstrates an effective methodology for mapping systems and structures for zoonotic diseases, and the benefit of conducting a baseline review of systemic capabilities prior to embarking on capacity building efforts.
more

The Leprosy Programme and Transmission Assessment (LPTA) is an activity that is carried out by internal teams towards the end of Phase 1 (see Leprosy Elimination Framework in the Annex) when a subnational jurisdiction (typically second-tier) reaches the milestone for interruption of transmission, i.
...
e., zero autochthonous child cases for a consecutive period of five years. It also needs to be done at the end of Phase 2, when the second milestone of elimination of leprosy disease has been reached. An LPTA will be carried out to document that all relevant programme criteria have been met and examine trends of epidemiological indicators in such jurisdiction to confirm that the milestone has been achieved. The LPTA includes assessment of health facilities that provide leprosy services. LPTA comprises of review of epidemiological data, health facility assessment and data validation and verification of the programme criteria through observation during a field visit. The evidence collected in this way in subnational health administrative units is compiled in a Leprosy Elimination Dossier to be submitted to WHO when the country reaches the milestone for elimination of disease in the country as whole. Countries that have not detected any new leprosy cases in the past three years or more can use the LPTA at national level prior to or as part of the verification process. Countries likely to be among the first to apply for verification may have had no new cases detected for more than 10 years.
more
The Leprosy Programme and Transmission Assessment (LPTA) is an activity that is carried out by internal teams towards the end of Phase 1 (see Leprosy Elimination Framework in the Annex) when a subnational jurisdiction (typically second-tier) reaches the milestone for interruption of transmission, i.
...
e., zero autochthonous child cases for a consecutive period of five years. It also needs to be done at the end of Phase 2, when the second milestone of elimination of leprosy disease has been reached. An LPTA will be carried out to document that all relevant programme criteria have been met and examine trends of epidemiological indicators in such jurisdiction to confirm that the milestone has been achieved. The LPTA includes assessment of health facilities that provide leprosy services. LPTA comprises of review of epidemiological data, health facility assessment and data validation and verification of the programme criteria through observation during a field visit. The evidence collected in this way in subnational health administrative units is compiled in a Leprosy Elimination Dossier to be submitted to WHO when the country reaches the milestone for elimination of disease in the country as whole. Countries that have not detected any new leprosy cases in the past three years or more can use the LPTA at national level prior to or as part of the verification process. Countries likely to be among the first to apply for verification may have had no new cases detected for more than 10 years.
more

Background
The ambitious development agenda of the Sustainable Development Goals (SDGs) requires substantial investments across several sectors, including for SDG 3 (healthy lives and wellbeing). No estimates of the additional resources needed to strengthen comprehensive health service delivery to
...
wards the attainment of SDG 3 and universal health coverage in low-income and middle-income countries have been published.
Methods
We developed a framework for health systems strengthening, within which population-level and individual-level health service coverage is gradually scaled up over time. We developed projections for 67 low-income and middle-income countries from 2016 to 2030, representing 95% of the total population in low-income and middle-income countries. We considered four service delivery platforms, and modelled two scenarios with differing levels of ambition: a progress scenario, in which countries’ advancement towards global targets is constrained by their health system’s assumed absorptive capacity, and an ambitious scenario, in which most countries attain the global targets. We estimated the associated costs and health effects, including reduced prevalence of illness, lives saved, and increases in life expectancy. We projected available funding by country and year, taking into account economic growth and anticipated allocation towards the health sector, to allow for an analysis of affordability and financial sustainability.
more

Trustworthy, evidence-based health guidelines form the basis of national policies affecting both patients and health-care workers. Emphasizing the link between robust evidence and people’s trust in their health systems, Dr Hans Henri P. Kluge, WHO Regional Director for Europe said at the launch ev
...
ent, “Trust and transformation are key words for us, especially when we talk about improving and strengthening our health systems. Transformation should first and foremost serve the interests of patients and health-care workers”.
While it is not always easy to demonstrate the immediate effect of guidelines on people’s health, there is no viable alternative to utilizing guidelines based on the best available evidence.
Yet, developing robust guidelines remains a challenge for most countries. “Guidelines need to be both simple to use and timely, they need to address people’s real needs, especially at the local level, and should ultimately reflect the resources available,” said Dr Natasha Azzopardi-Muscat, Director, Country Health Policies and Systems, WHO/Europe. “This means that any successful guideline needs to be adjusted and adapted to local contexts and realities.”
more

The WHO Global Antimicrobial Resistance and Use Surveillance System (GLASS) was launched in 2015 to foster AMR surveillance and inform strategies to contain AMR. The system started with surveillance of AMR in bacteria causing common human infections and has expanded its scope to include surveillance
...
of antimicrobial consumption (AMC), invasive fungal infections, and a One Health surveillance model relevant to human health. To meet future challenges, it is in continuous evolution to enhance the quality and representativeness of data to inform the AMR burden accurately. As of the end of 2022, 127 countries, territories and areas participate in GLASS.
The fifth GLASS report, produced in collaboration with Member States, summarizes 2020 data on AMR rates in common bacteria from countries, territories, and areas. The report brings new features, including analyses of population testing coverage or AMR trends. For the first time, the report presents 2020 data on AMC at the national level. A new interactive dashboard allow users to explore AMR and AMC global data, country profiles and download the data.
This report marks the end of the early implementation phase of GLASS. In addition to presenting data collected through the latest data call, this report provides a summary of five years of national AMR surveillance data contributed to GLASS from its initiation, presents AMR findings in the context of progress of country participation in GLASS and in global AMR surveillance coverage and laboratory quality assurance systems at (sub)national level.
Patterns of antimicrobial consumption are presented by country with a particular focus on antibacterials. The report also presents the antimicrobial consumption according to the WHO AWaRe antibiotic classification, for penicillins and cephalosporines. From a One Health perspective, the report presents antimicrobial consumption data in the human sector expressed in tons to allow a comparison with antimicrobial consumption from other sectors (not included in this report).
more