Filter
53
Featured
7
16
Language
Document type
26
11
5
4
4
2
1
Countries
5
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Toolboxes
16
5
2
1

Vía clínica

Hypertension, or high blood pressure, is a condition which generally has no symptoms and if left untreated, can lead to heart attacks, heart failure, stroke, kidney failure and blindness. Risk factors include older age, overweight or obesity, lack of physical activity, high salt/sodium intake, and h
...

Vía Clínica de Hipertensión

This report compiles data for the first time on the far-reaching consequences of uncontrolled hypertension, including heart attacks, strokes and premature death, along with substantial economic losses for communities and countries. It also contains information on the global, regional and country-lev
...
Cardiovascular disease (CVD) is the leading cause of death in the Americas and raised blood pressure accounts for over 50% of CVD. In the Americas over a quarter of adult women and four in ten adult men have hypertension and the diagnosis, treatment and control are suboptimal. In 2021, the World Hea
...
Myocardial infarctions are generally clinically classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI), based on changes in ECG. When blood flow to a part of the heart stops or the heart is injured and fails to receive enough oxygen required for its adequate functioning the conditi
...
Scientific Brief, 17 June 2021

WHO list of priority medical devices for management of cardiovascular diseases and diabetes
recommended
This publication was developed in response to the need for a reference list of priority medical devices required for management of noncommunicable diseases (NCDs), focusing on cardiovascular diseases and diabetes, especially for low- and middle-income countries to support universal health coverage a
...

This toolkit was developed by the Centers for Disease Control and Prevention (CDC) Division for Heart Disease and Stroke Prevention (DHDSP) to provide healthcare organizations, including those in resource-constrained settings, with the information and resources to implement the HMP and improve hyper
...
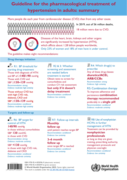
The recommendations cover the level of blood pressure to start medication, what type of medicine or combination of medicines to use, the target blood pressure level, and how often to have follow-up checks on blood pressure. In addition, the guideline provides the basis for how physicians and other h
...

Note d’information scientifique, 17 juin 2021


The recommendations cover the level of blood pressure to start medication, what type of medicine or combination of medicines to use, the target blood pressure level, and how often to have follow-up checks on blood pressure. In addition, the guideline provides the basis for how physicians and other h
...
Mais pessoas morrem a cada ano de doenças cardiovasculares do que de qualquer outra causa. Mais de três quartos das mortes por doenças cardíacas e acidentes vasculares cerebrais ocorrem em países de baixa e média renda. A hipertensão - ou pressão alta - é uma condição médica grave que au
...
Hypertension is referred to as a “silent killer”. Most people with hypertension are unaware of their condition as in most cases, they experience no warning signs or symptoms hence they are not identified or treated. Hypertention is associated with a number of conditions, disability, and causes o
...

The South African (SA) guidelines for cardiac patients for non-cardiac surgery were developed to address the need for cardiac risk assessment and risk stratification for elective non-cardiac surgical patients in SA, and more broadly in Africa.
The guidelines were developed by updating the Canadian
...
Primary care health centers and providers who care for individuals with hypertension and cardiovascular disease have an important role to play in ensuring continued access to care, reducing the risk of coronavirus infection, and appropriately managing people with these co-morbidities who acquire COV
...
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV‑2) causing coronavirus disease 2019 (COVID-19) has reached pandemic levels;
Patients with cardiovascular (CV) risk factors and established cardiovascular disease (CVD) represent a vulnerable population when suffering from COVID-19;
Patien
...
second edition
Included more self-measured blood pressure (SMBP)-focused content with tools and resources.
Showcased more tools to find patients with potentially undiagnosed HTN.
Added new strategies that focus on chronic kidney disease testing and identification.