Filter
201
Featured
1
6
Language
Document type
85
30
21
18
12
9
8
6
5
3
1
1
1
1
Countries
18
13
11
8
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
80
41
39
18

Many low- and middle-income countries (LMICs) are undergoing an epidemiological transition. With an improvement in socioeconomic conditions and an aging population, cardiovascular diseases (CVDs), like cardiac arrhythmias, are expected to increase in these countries. However, there are limited studi
...
Socioeconomic status is associated with differences in risk factors for cardiovascular disease incidence and outcomes, including mortality. However, it is unclear whether the associations between cardiovascular disease and common measures of socioeconomic status—wealth and education—differ among
...

Outdoor air pollution is one of the world's largest health and environmental problems. The Global Burden of Disease is a major global study on the causes and risk factors for death. These estimates of the annual number of deaths attributed to a wide range of risk factors are shown here. This chart i
...
Cardiovascular diseases (CVDs) are a growing public health problem in Ghana and other African countries. Strokes and other CVDs have become a leading cause of death due to increasing risk factors such as hypertension. According to the Global Burden of Disease study (GBD), ischaemic heart disease was
...
troke, a major Non-Communicable Disease (NCD), is responsible for 3.5% of disabilityadjusted life year (DALY) in India.Apart from risk factors like hypertension, diabetes, heart diseases and positive family history, other lifestyle related factors such as unhealthy diet, obesity, lack of physical ac
...

In many low- and middle-income countries, there is a wide gap between evidencebased recommendations and current practice. Treatment of major CVD risk factors remains suboptimal, and only a minority of patients who are treated reach their target levels for blood pressure, blood sugar and blood choles
...

Procurement and supply management activities are fundamental to consistent and reliable access to essential medicines and health products. To reduce the impact of CVD, action needs to be taken to improve prevention, diagnosis, care and management of CVD diseases. Affordable essential medicines and t
...

Many low-resource settings have a shortage of physicians and health workers. (1) In order to provide patient-centred continuous care more effectively, primary care systems can include team-based care strategies in their clinic workflows and protocols. Team-based care uses multidisciplinary teams (wh
...

Monitoring is a crucial element in any successful programme. It is important to
know if health care facilities – and ultimately countries – are meeting the agreed
goals and objectives for preventing and managing cardiovascular diseases (CVD).
Monitoring is the on-going collection, management
...

HEARTS provides a set of locally adaptable tools for strengthening the
management of CVD in primary health care.
HEARTS is designed to enhance implementation of WHO PEN by providing:
• operational guidance on further integrating CVD management
• technical guidance on evaluating the impact of
...

Technical package for cardiovascular disease management in primary health care.

The risk factors for CVD include behavioural factors, such as tobacco use, an unhealthy diet, harmful use of alcohol and inadequate physical activity, and physiological (metabolic) factors, including high blood pressure (hypertension), high blood cholesterol and high blood sugar or glucose. Both kin
...
Many features of the environment have been found to exert an important influence on cardiovascular disease (CVD) risk, progression, and severity. Changes in the environment due to migration to different geographic locations, modifications in lifestyle choices, and shifts in social policies and cultu
...
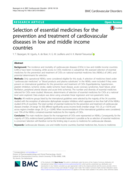
The incidence and mortality of cardiovascular diseases (CVDs) in low and middle income countries (LMICs) have been increasing, while access to CVDs medicines is suboptimal. We assessed selection of essential medicines for the prevention and treatment of CVDs on national essential medicines lists (NE
...
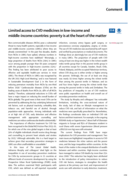
Non-communicable diseases (NCDs) pose a substantial threat to many health systems, especially in low-income and middle-income countries (LMICs) where they are already overstretched. In the past few decades, deaths from NCDs in LMICs have spiked, whereas numbers in high-income countries have stabilis
...
The Kenya Health Policy 2014-2030 aims at attaining the highest possible standard of health in a manner responsive to the health needs of our population. One of the major policy directions towards realizing the intentions of this policy is to halt and reverse the
rising burden of non-communicable d
...

Introduction Community health workers (CHWs) are increasingly being tasked to prevent and manage cardiovascular disease (CVD) and its risk factors in underserved populations in low-income and middle-income countries (LMICs); however, little is known about the required training necessary for them to
...

INTRODUCTION: Lower extremity peripheral artery disease (PAD) is increasing in prevalence in low- and middle-income countries creating a large health care burden. Clinical management may require substantial resources but little consideration has been given to which treatments are appropriate for les
...

This is an update (third edition) of the BACPR Standards & Core Components and represents current evidence-based best practice and a pragmatic overview of the structure and function of Cardiovascular Prevention and Rehabilitation Programmes (CPRPs) in the UK. The previously described seven standards
...

Hypertension is the number one health related risk factor in India, with the largest contribution to burden of disease and mortality. It contributes to an estimated 1.6 million deaths, due to ischemic heart disease and stroke, out of a total of about 10 million deaths annually in India. Fifty seven
...