Filter
178
Text search:
buruli
ulcer
Featured
26
21
Language
Document type
58
39
24
14
9
8
7
5
5
5
4
Countries
14
6
6
5
3
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
34
25
8
4
4
3
1
Toolboxes
116
6
3
3
2
2
1
1
1
1
1
1
1
1
1
Key facts
Buruli ulcer is a chronic debilitating disease caused by an environmental Mycobacterium ulcerans.
At least 33 countries with tropical, subtropical and temperate climates have reporte
...
Website last accessed on 18.03.2023
Website last accessed on 18.03.2023
The GHO data repository is WHO's gateway to health-related statistics for its 194 Member States. It provides access to over 1000 health topics indicators.
Website last accessed on 18.03.2023
Early detection of cases is critical to complete cure with combined antibiotics. In its late stages, Buruli ulcer causes severe destruction of the skin, leading
...
Buruli ulcer is a disease of skin and soft tissue with the potential to leave sufferers scarred and disabled. It is caused by an environmental pathogen, Mycobacterium
ulcerans, that produces a des
...
Website - last accessed on 18.03.2023

Website last accessed on 18.03.2023
Buruli Ulcer Disease: Obtaining Swab Specimens for Diagnosis of M. Ulcerans Infection - Youtube video

MEDBOX Issue Brief no.35: The first issue brief on the NTD Toolbox contains general strategies, roadmaps, key treatment guidelines, reports, and training material on Buruli ulcer, Chagas, and Leishm
...
Buruli ulcer is a disease caused by the environmental pathogen Mycobacterium ulcerans that affects skin and soft tissue. It was first described in Australia in 1948 and has been reported in several
...

Data available for your search include drug targets, tested compounds, existing drugs, ethnopharmacological plants, and information on the genome of M. ulcerans
Dermatologic Clinics Volume 29, Issue 1p1-8January 2011
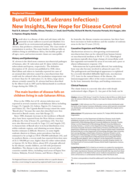
A review of prospects for existing antibiotics ad new therapeutics
In the 126 years since it was first described, scientists have learned a great deal about Buruli ulcer, (an ulcerating skin infection caused by the environmental bacterium, Mycobacterium ulcerans),
...
The Lancet Volume 399, Issue 10327p786-797February 26, 2022
Free download after free registration

Journal of Computational Biophysics and ChemistryVol. 22, No. 01, pp. 31-41 (2023)

Buruli ulcer (BU), a neglected tropical disease (NTD), is an infection of the skin and subcutaneous tissue caused by Mycobacterium ulcerans. The disease has been documented in many South American,
...
Status of endemicity of Buruli ulcer 2023
Although Buruli ulcer, tuberculosis, and leprosy are the three most common mycobacterial diseases, One Health dimensions of these infections remain poorly understood. This narrative review aims at e
...
Buruli ulcer (BU), the second most common mycobacterial disease in West Africa, is a necrotizing skin disease that can lead to high morbidity in affected patients. The disease is caused by Mycobacte
...