buruli ulcer
Als docx, pdf herunterladen1 gefällt mir985 aufrufe
Buruli ulcer is a disease caused by the environmental pathogen Mycobacterium ulcerans that affects skin and soft tissue. It was first described in Australia in 1948 and has been reported in several sub-Saharan African countries since the late 19th century. The disease mainly affects children in rural areas and causes lesions and ulcers that can lead to disability if not treated. Recent research has identified a toxin produced by M. ulcerans that may be responsible for the disease's pathogenesis. Efforts are ongoing to understand transmission and develop effective control strategies, including through training of medical professionals and increased detection and treatment of cases.
1 von 4
11-mal heruntergeladen


Anzeige
Empfohlen
Japanese encephalitis
Japanese encephalitis Nikkin T Japanese encephalitis is a mosquito-borne viral disease that is common in parts of Asia. It is transmitted to humans via bites from infected Culex mosquitoes. While most infections cause mild symptoms or no symptoms, approximately 1 in 250 infections result in encephalitis, which can be fatal in 30% of cases. Survivors often face permanent neurological impairments. Control efforts focus on vaccination programs and reducing mosquito populations in areas like rice paddies where they breed.
Dengue
DengueSachin Verma Dengue fever, caused by the dengue virus transmitted by Aedes aegypti mosquitoes, presents various clinical manifestations including undifferentiated fever, classic dengue fever, and dengue hemorrhagic fever (DHF). Key diagnostic criteria for DHF include fever, hemorrhagic manifestations, and low platelet count, while management focuses on hydration and monitoring for severe complications. Effective vector control strategies are crucial for preventing outbreaks, emphasizing the need for environmental management and targeted interventions.
Shingles
Shinglesfitango Shingles, or herpes zoster, affects about 1 million people in the U.S. annually, primarily those over 50 or with weakened immune systems due to various conditions. Caused by the varicella-zoster virus, the disease can present with early symptoms of pain and a subsequent rash, requiring diagnosis and treatment from healthcare providers. While there is no cure, antiviral medications can lessen the severity and duration of the attack, and vaccination is recommended for those 60 and older to reduce incidence and severity.
Epidemiology and control of filariasis (Lymphatic Filariasis) in India
Epidemiology and control of filariasis (Lymphatic Filariasis) in IndiaReshma Ann Mathew Lymphatic filariasis is a major public health problem in India, caused by parasitic filarial worms transmitted by mosquitoes. It manifests as lymphedema, elephantiasis, and hydrocele. Mass drug administration of diethylcarbamazine is used for treatment and control. Vector control via reducing mosquito breeding also helps control transmission. The goal is to eliminate the disease as a public health problem by 2020 through interrupting transmission. Assessment involves monitoring microfilaria rates, disease prevalence, and entomological parameters to evaluate control programs.
Presentation On Buruli Ulcer
Presentation On Buruli UlcerABURA Foundation Buruli ulcer is a devastating skin disease caused by Mycobacterium ulcerans that affects skin and soft tissue. It was first reported in Uganda in 1961 and is common near rivers and slow-moving bodies of water. The exact transmission is unknown but may involve mosquitoes. Treatment involves antibiotics for 8 weeks and sometimes surgery. Early detection and treatment are important to prevent disability and long-term functional limitations like joint restrictions. Control strategies focus on community education, healthcare worker training, and standardized case management and reporting.
Filariasis
�
Filariasis
�Society for Microbiology and Infection care Lymphatic filariasis, also known as elephantiasis, is caused by parasitic roundworms that are spread by mosquitoes and black flies. It affects over 120 million people worldwide. The parasites block the lymphatic system leading to swelling in the limbs and genitals. Diagnosis was difficult previously but can now be made through blood tests that detect parasites or antibodies. While some infected individuals show no symptoms, others develop severe elephantiasis characterized by thickening of the skin and limbs. Treatment aims to eliminate parasites and prevent further transmission and symptoms.
Poliomyelitis
PoliomyelitisLiezle Joy Gargoles Poliomyelitis is an infectious disease caused by a poliovirus that primarily affects the spinal cord. It was once a global disease but through vaccination efforts, now only exists in a few countries in Africa and Asia. The virus is transmitted via the fecal-oral route. It enters the body through the mouth and may cause a range of symptoms from none to paralysis depending on if it infects the spinal cord. Treatment focuses on symptoms and rehabilitation while vaccination is the best prevention method.
Tuberculous meningitis
Tuberculous meningitiszahid mehmood Tuberculous meningitis is inflammation of the membranes surrounding the brain and spinal cord caused by Mycobacterium tuberculosis. It typically develops secondary to a pulmonary tuberculosis infection. Symptoms progress through three stages - an initial prodromal stage with nonspecific symptoms, followed by signs of meningeal irritation and cranial nerve palsies, and finally a terminal stage with coma and death if untreated. Diagnosis involves lumbar puncture showing lymphocytic pleocytosis and decreased glucose. Treatment consists of a combination of antitubercular drugs for 12 months along with corticosteroids to reduce inflammation and complications. Prognosis depends on the stage of disease at treatment initiation, with mortality rates as high as 50%
Dengue fever
Dengue feverMedical Knowledge Dengue fever is a mosquito-borne tropical disease caused by the dengue virus. It is transmitted by Aedes mosquitoes, most commonly A. aegypti. Symptoms include high fever, headache, muscle and joint pains, and a skin rash. In severe cases it can develop into life-threatening dengue hemorrhagic fever or dengue shock syndrome. There is no vaccine, so prevention focuses on controlling mosquito habitats and limiting exposure to bites. Treatment involves fluid replacement and blood transfusion in severe cases.
Amputations
AmputationsRatan Khuman The document discusses the history and process of amputation. It traces the etymology of the word "amputation" back to Latin and describes its early uses. It then covers the development of amputation techniques throughout history. The document also defines types of amputations, common causes, and potential complications. It provides details on the principles and process of both closed and open amputations.
Filariasis
Filariasisprakashtu This document provides an overview of filariasis (lymphatic filariasis). It begins with an introduction and outlines the topics to be covered, which include epidemiology, morphology, transmission, life cycle, pathogenesis, diagnosis, prevention and control. It then delves into each topic in detail. Some key points are: lymphatic filariasis is caused by infection with filarial nematodes and transmitted by mosquitoes; it affects over 120 million people globally, with highest prevalence in South and Southeast Asia and Africa; microscopic examination of blood and tissue samples is used for diagnosis; prevention focuses on vector control and treatment includes drugs to kill worms and parasites.
Leprosy
LeprosyAmal Osman Leprosy is caused by Mycobacterium leprae, an acid-fast bacillus. It primarily affects the skin and peripheral nerves, causing sensory loss and disability if left untreated. While only a small portion of those exposed develop clinical disease, transmission occurs through droplets from the nose and mouth. Treatment involves multidrug therapy with dapsone, rifampicin, and clofazimine, which cures the disease and eliminates infectivity. Control relies on early diagnosis and treatment to prevent disability, along with health education to reduce stigma. Global efforts have led to the elimination of leprosy as a public health problem.
Polio
PolioDr. Vyom Jain The document provides an overview of poliomyelitis, including its historical context, causes, transmission, symptoms, and treatment options. It details the types of poliovirus, the classification of polio infections, and potential complications, as well as rehabilitation strategies for affected individuals. The document also highlights the importance of awareness and efforts towards global polio eradication.
Complications of fractures
Complications of fracturesSubhanjan Das The document discusses various pathologies that can occur with fractures beyond just the bone break itself. It classifies complications as immediate, early, or late and discusses specific issues like hypovolamic shock, fat embolism, deep vein thrombosis, crush syndrome, compartment syndrome, and delayed or non-union. Treatment options are provided for many of these complications aiming to address the underlying causes and minimize long-term disabilities. Early diagnosis and aggressive management of fractures and their associated issues is emphasized.
Malaria ppt
Malaria pptJegon Varakala Malaria remains a devastating global health issue, infecting hundreds of millions annually. It is caused by Plasmodium parasites and transmitted via Anopheles mosquitoes. The malaria lifecycle involves both asexual and sexual reproduction in the human and mosquito hosts. In humans, the parasites multiply in the liver and infect red blood cells, causing symptoms like fever, chills, and headaches in cycles. Untreated, P. falciparum malaria can cause severe complications like cerebral malaria. Diagnosis involves examining blood films microscopically or using rapid tests to detect parasites or antigens. While some drugs like chloroquine once treated malaria, resistance requires newer combinations of artemisinin with other therapies for effective treatment.
Orchitis & epididymitis
Orchitis & epididymitisKaey Shins This document provides information about orchitis, including its causes, symptoms, diagnosis, and treatment. Orchitis is an inflammation of the testicles that is usually caused by a virus like mumps or bacteria that spreads from an associated epididymitis. Common symptoms include pain and tenderness in the testicles and scrotum. Diagnosis involves examination of the testicles and scrotum along with potential laboratory tests. While viral orchitis cannot be cured, it will resolve on its own. Bacterial orchitis is treated with antibiotics and anti-inflammatory medications.
HIV infection (AIDS)
HIV infection (AIDS)Namrata Chhabra AIDS is a syndrome caused by HIV that leads to severe immune system damage, making individuals susceptible to various infections and cancers. HIV, discovered in 1981, has a global prevalence, with approximately 40 million people infected. The virus primarily targets CD4 T lymphocytes, and its transmission occurs through sexual contact, blood transfusion, and from mother to child, with a significant reduction in mortality due to antiretroviral therapy.
MEASLES
MEASLESAl-YAQIN DIAGNOSTIC ULTRASONIC CLINIC BAGHDAD Measles is a highly contagious viral infection with significant historical impacts, causing millions of deaths worldwide before vaccination. It is characterized by symptoms such as fever, cough, coryza, conjunctivitis, and a distinctive maculopapular rash. While there is no specific antiviral treatment, supportive care and vaccination are key in prevention and management of the disease.
Bone tumors
Bone tumorsBADAL BALOCH The document provides an overview of bone tumors, categorizing them into primary and secondary tumors, with further classifications for benign and malignant types. It discusses the most common types of tumors, their characteristics, symptoms, imaging findings, and staging systems for treatment purposes. Treatment options vary, emphasizing surgical excision and, in some cases, chemotherapy, depending on the tumor type and stage.
Leishmaniasis (Kala Azar)
Leishmaniasis (Kala Azar)Dr. Samarjeet Kaur This document discusses leishmaniasis, a parasitic disease transmitted by sandflies. It causes visceral leishmaniasis (kala azar), cutaneous leishmaniasis, and mucocutaneous leishmaniasis. India has the highest burden of visceral leishmaniasis globally, with Bihar being the most affected state. The parasite infects macrophages and clinical features include irregular fever, weight loss, hepatosplenomegaly, and anemia. Diagnosis involves identifying the parasite in tissue aspirates or using serological tests. Treatment options include pentavalent antimony, pentamidine, amphotericin B, and miltefosine. Control relies on
Infectious mononucleosis
Infectious mononucleosisVasyl Sorokhan This document summarizes key information about infectious mononucleosis caused by Epstein-Barr virus (EBV). It was first described in 1920 and causes fever, pharyngitis, and adenopathy. Diagnosis involves detecting heterophile antibodies or testing for EBV-specific antibodies. Physical exam may show lymphadenopathy, hepatosplenomegaly, or periorbital edema. Laboratory tests include complete blood count showing lymphocytosis and atypical lymphocytes as well as elevated liver enzymes. Specific antibody testing confirms diagnosis and distinguishes between acute and past EBV infection.
Lymphatic Filariasis jp
Lymphatic Filariasis jpRangineni Prada Lymphatic filariasis is caused by infection with filarial nematodes transmitted by mosquitoes. It affects over 120 million people globally. The parasites Wuchereria bancrofti, Brugia malayi and Brugia timori develop through larvae stages in mosquitoes before infecting humans via mosquito bites. The adult worms live in the lymphatic vessels and cause lymphangitis and lymph node obstruction, leading to lymphedema and elephantiasis. Microfilariae are periodic in the blood and can be diagnosed via blood smears. There is no treatment for established disease but prevention focuses on mass drug administration.
Acute encephalitis suresh ppt
Acute encephalitis suresh pptBhargav Kiran This document discusses acute encephalitis in India. It defines acute encephalitis and acute encephalitis syndrome. Japanese encephalitis virus is a major cause of AES in India, transmitted via Culex mosquitoes between pigs, birds and humans. The document outlines the epidemiology, clinical features, diagnosis and management of AES. It emphasizes the importance of vaccination and vector control in prevention and control of AES in India.
Lathyrus sativus - a path to Neurolathyrism
Lathyrus sativus - a path to Neurolathyrism Maheshwor Yadav Lathyrus sativus, commonly known as khesari dal, is a nutritious but potentially harmful legume due to the presence of the neurotoxin ODAP, which can cause neurolathyrism, a neurological disorder characterized by paralysis of the lower limbs. This condition typically arises during periods of famine when Lathyrus sativus becomes a staple food, and symptoms are irreversible once they appear. Although efforts have been made to mitigate this issue through food processing and regulation, the disease persists in certain regions, necessitating a balanced approach to its cultivation and consumption.
Inactivated polio vaccine(IPV)
Inactivated polio vaccine(IPV)AishwaryaRG2 The document summarizes key information about inactivated polio vaccine (IPV), including that it is made from killed poliovirus strains, it produces antibodies but not intestinal immunity, it requires multiple doses for protection, and it carries no risk of vaccine-associated paralysis unlike the live oral polio vaccine (OPV). IPV is recommended for routine use in industrialized countries where the risk of vaccine-derived polio is greater than wild poliovirus, while OPV is used to contain outbreaks and in immunization programs in developing countries.
Hypertension Community Medicine Presentation
Hypertension Community Medicine PresentationAdwaithA2 Hypertension is a prevalent cardiovascular disorder that poses significant health risks, including coronary heart disease and stroke, affecting a substantial portion of the global population. It is classified into primary (essential) and secondary hypertension, with modifiable and non-modifiable risk factors contributing to its prevalence, which can reach over 60% in older adults. Effective prevention and management strategies focus on lifestyle modifications, early detection, and patient compliance to reduce blood pressure and associated health complications.
Complications of malaria
Complications of malariaChandan N Cerebral malaria is a serious complication of Plasmodium falciparum infection that commonly affects children and non-immune adults, causing decreased consciousness ranging from drowsiness to coma. Late stage parasites cause aggregation of red blood cells in the brain, leading to capillary plugging, anoxia, and hemorrhage. Renal failure is also common, resulting from deposition of hemoglobin in renal tubules and decreased blood flow. Other complications include non-cardiogenic pulmonary edema, hypoglycemia from hepatic dysfunction, acidosis, anemia, thrombocytopenia, and jaundice. Chronic complications include tropical splenomegaly and quartan malarial nephropathy.
History and examination in orthopedics
History and examination in orthopedicsSalar Jakhsi Orthopedic surgeons deal with diseases and injuries of the musculoskeletal system. Diagnosis depends on taking a thorough history, conducting a physical examination, and ordering investigations. The history focuses on personal details, chief complaints, present illness, past medical history, medications, family history, and social history. The physical examination involves inspecting, feeling, and moving the affected area as well as conducting neurovascular and special tests. Imaging studies like x-rays, CT scans, MRIs, and scans are important investigations to diagnose orthopedic conditions.
Competition Journal Article by Emilio Varanini and Feng Jiang
Competition Journal Article by Emilio Varanini and Feng JiangEmilio Varanini This document summarizes a 2014 Chinese Supreme Court decision regarding antitrust law between Qihoo and Tencent. It discusses how the decision demonstrates China's commitment to developing the rule of law in several ways:
1) By thoroughly applying legal principles and economic theories to complex factual circumstances, helping to balance administrable rules with economic analysis.
2) By establishing an important precedent that lower courts can apply to similar cases, developing China's system of case law.
3) By following due process and protecting the legitimate interests of litigants.
The document argues this decision shows the Chinese judiciary is capable of carrying out the tasks necessary for the rule of law, and its influence will depend on how
Esei masy agraria belanda
Esei masy agraria belandaMargaret Denny Masyarakat agraria di Belanda pada abad ke-16 hingga ke-17 ditandai dengan kegiatan pertanian dan penternakan, yang meningkat akibat revolusi pertanian dan teknologi baru seperti kincir angin. Mereka terkenal dengan pengeluaran tanaman bijirin, industri tekstil, dan penangkapan ikan, serta menjadi pusat utama penternakan lembu tenusu. Ekonomi Belanda mencapai puncak pada abad ke-17, tetapi mulai mengalami kemerosotan pada awal abad ke-18 disebabkan persaingan internasional.
Weitere ähnliche Inhalte
Was ist angesagt? (20)
Dengue fever
Dengue feverMedical Knowledge Dengue fever is a mosquito-borne tropical disease caused by the dengue virus. It is transmitted by Aedes mosquitoes, most commonly A. aegypti. Symptoms include high fever, headache, muscle and joint pains, and a skin rash. In severe cases it can develop into life-threatening dengue hemorrhagic fever or dengue shock syndrome. There is no vaccine, so prevention focuses on controlling mosquito habitats and limiting exposure to bites. Treatment involves fluid replacement and blood transfusion in severe cases.
Amputations
AmputationsRatan Khuman The document discusses the history and process of amputation. It traces the etymology of the word "amputation" back to Latin and describes its early uses. It then covers the development of amputation techniques throughout history. The document also defines types of amputations, common causes, and potential complications. It provides details on the principles and process of both closed and open amputations.
Filariasis
Filariasisprakashtu This document provides an overview of filariasis (lymphatic filariasis). It begins with an introduction and outlines the topics to be covered, which include epidemiology, morphology, transmission, life cycle, pathogenesis, diagnosis, prevention and control. It then delves into each topic in detail. Some key points are: lymphatic filariasis is caused by infection with filarial nematodes and transmitted by mosquitoes; it affects over 120 million people globally, with highest prevalence in South and Southeast Asia and Africa; microscopic examination of blood and tissue samples is used for diagnosis; prevention focuses on vector control and treatment includes drugs to kill worms and parasites.
Leprosy
LeprosyAmal Osman Leprosy is caused by Mycobacterium leprae, an acid-fast bacillus. It primarily affects the skin and peripheral nerves, causing sensory loss and disability if left untreated. While only a small portion of those exposed develop clinical disease, transmission occurs through droplets from the nose and mouth. Treatment involves multidrug therapy with dapsone, rifampicin, and clofazimine, which cures the disease and eliminates infectivity. Control relies on early diagnosis and treatment to prevent disability, along with health education to reduce stigma. Global efforts have led to the elimination of leprosy as a public health problem.
Polio
PolioDr. Vyom Jain The document provides an overview of poliomyelitis, including its historical context, causes, transmission, symptoms, and treatment options. It details the types of poliovirus, the classification of polio infections, and potential complications, as well as rehabilitation strategies for affected individuals. The document also highlights the importance of awareness and efforts towards global polio eradication.
Complications of fractures
Complications of fracturesSubhanjan Das The document discusses various pathologies that can occur with fractures beyond just the bone break itself. It classifies complications as immediate, early, or late and discusses specific issues like hypovolamic shock, fat embolism, deep vein thrombosis, crush syndrome, compartment syndrome, and delayed or non-union. Treatment options are provided for many of these complications aiming to address the underlying causes and minimize long-term disabilities. Early diagnosis and aggressive management of fractures and their associated issues is emphasized.
Malaria ppt
Malaria pptJegon Varakala Malaria remains a devastating global health issue, infecting hundreds of millions annually. It is caused by Plasmodium parasites and transmitted via Anopheles mosquitoes. The malaria lifecycle involves both asexual and sexual reproduction in the human and mosquito hosts. In humans, the parasites multiply in the liver and infect red blood cells, causing symptoms like fever, chills, and headaches in cycles. Untreated, P. falciparum malaria can cause severe complications like cerebral malaria. Diagnosis involves examining blood films microscopically or using rapid tests to detect parasites or antigens. While some drugs like chloroquine once treated malaria, resistance requires newer combinations of artemisinin with other therapies for effective treatment.
Orchitis & epididymitis
Orchitis & epididymitisKaey Shins This document provides information about orchitis, including its causes, symptoms, diagnosis, and treatment. Orchitis is an inflammation of the testicles that is usually caused by a virus like mumps or bacteria that spreads from an associated epididymitis. Common symptoms include pain and tenderness in the testicles and scrotum. Diagnosis involves examination of the testicles and scrotum along with potential laboratory tests. While viral orchitis cannot be cured, it will resolve on its own. Bacterial orchitis is treated with antibiotics and anti-inflammatory medications.
HIV infection (AIDS)
HIV infection (AIDS)Namrata Chhabra AIDS is a syndrome caused by HIV that leads to severe immune system damage, making individuals susceptible to various infections and cancers. HIV, discovered in 1981, has a global prevalence, with approximately 40 million people infected. The virus primarily targets CD4 T lymphocytes, and its transmission occurs through sexual contact, blood transfusion, and from mother to child, with a significant reduction in mortality due to antiretroviral therapy.
MEASLES
MEASLESAl-YAQIN DIAGNOSTIC ULTRASONIC CLINIC BAGHDAD Measles is a highly contagious viral infection with significant historical impacts, causing millions of deaths worldwide before vaccination. It is characterized by symptoms such as fever, cough, coryza, conjunctivitis, and a distinctive maculopapular rash. While there is no specific antiviral treatment, supportive care and vaccination are key in prevention and management of the disease.
Bone tumors
Bone tumorsBADAL BALOCH The document provides an overview of bone tumors, categorizing them into primary and secondary tumors, with further classifications for benign and malignant types. It discusses the most common types of tumors, their characteristics, symptoms, imaging findings, and staging systems for treatment purposes. Treatment options vary, emphasizing surgical excision and, in some cases, chemotherapy, depending on the tumor type and stage.
Leishmaniasis (Kala Azar)
Leishmaniasis (Kala Azar)Dr. Samarjeet Kaur This document discusses leishmaniasis, a parasitic disease transmitted by sandflies. It causes visceral leishmaniasis (kala azar), cutaneous leishmaniasis, and mucocutaneous leishmaniasis. India has the highest burden of visceral leishmaniasis globally, with Bihar being the most affected state. The parasite infects macrophages and clinical features include irregular fever, weight loss, hepatosplenomegaly, and anemia. Diagnosis involves identifying the parasite in tissue aspirates or using serological tests. Treatment options include pentavalent antimony, pentamidine, amphotericin B, and miltefosine. Control relies on
Infectious mononucleosis
Infectious mononucleosisVasyl Sorokhan This document summarizes key information about infectious mononucleosis caused by Epstein-Barr virus (EBV). It was first described in 1920 and causes fever, pharyngitis, and adenopathy. Diagnosis involves detecting heterophile antibodies or testing for EBV-specific antibodies. Physical exam may show lymphadenopathy, hepatosplenomegaly, or periorbital edema. Laboratory tests include complete blood count showing lymphocytosis and atypical lymphocytes as well as elevated liver enzymes. Specific antibody testing confirms diagnosis and distinguishes between acute and past EBV infection.
Lymphatic Filariasis jp
Lymphatic Filariasis jpRangineni Prada Lymphatic filariasis is caused by infection with filarial nematodes transmitted by mosquitoes. It affects over 120 million people globally. The parasites Wuchereria bancrofti, Brugia malayi and Brugia timori develop through larvae stages in mosquitoes before infecting humans via mosquito bites. The adult worms live in the lymphatic vessels and cause lymphangitis and lymph node obstruction, leading to lymphedema and elephantiasis. Microfilariae are periodic in the blood and can be diagnosed via blood smears. There is no treatment for established disease but prevention focuses on mass drug administration.
Acute encephalitis suresh ppt
Acute encephalitis suresh pptBhargav Kiran This document discusses acute encephalitis in India. It defines acute encephalitis and acute encephalitis syndrome. Japanese encephalitis virus is a major cause of AES in India, transmitted via Culex mosquitoes between pigs, birds and humans. The document outlines the epidemiology, clinical features, diagnosis and management of AES. It emphasizes the importance of vaccination and vector control in prevention and control of AES in India.
Lathyrus sativus - a path to Neurolathyrism
Lathyrus sativus - a path to Neurolathyrism Maheshwor Yadav Lathyrus sativus, commonly known as khesari dal, is a nutritious but potentially harmful legume due to the presence of the neurotoxin ODAP, which can cause neurolathyrism, a neurological disorder characterized by paralysis of the lower limbs. This condition typically arises during periods of famine when Lathyrus sativus becomes a staple food, and symptoms are irreversible once they appear. Although efforts have been made to mitigate this issue through food processing and regulation, the disease persists in certain regions, necessitating a balanced approach to its cultivation and consumption.
Inactivated polio vaccine(IPV)
Inactivated polio vaccine(IPV)AishwaryaRG2 The document summarizes key information about inactivated polio vaccine (IPV), including that it is made from killed poliovirus strains, it produces antibodies but not intestinal immunity, it requires multiple doses for protection, and it carries no risk of vaccine-associated paralysis unlike the live oral polio vaccine (OPV). IPV is recommended for routine use in industrialized countries where the risk of vaccine-derived polio is greater than wild poliovirus, while OPV is used to contain outbreaks and in immunization programs in developing countries.
Hypertension Community Medicine Presentation
Hypertension Community Medicine PresentationAdwaithA2 Hypertension is a prevalent cardiovascular disorder that poses significant health risks, including coronary heart disease and stroke, affecting a substantial portion of the global population. It is classified into primary (essential) and secondary hypertension, with modifiable and non-modifiable risk factors contributing to its prevalence, which can reach over 60% in older adults. Effective prevention and management strategies focus on lifestyle modifications, early detection, and patient compliance to reduce blood pressure and associated health complications.
Complications of malaria
Complications of malariaChandan N Cerebral malaria is a serious complication of Plasmodium falciparum infection that commonly affects children and non-immune adults, causing decreased consciousness ranging from drowsiness to coma. Late stage parasites cause aggregation of red blood cells in the brain, leading to capillary plugging, anoxia, and hemorrhage. Renal failure is also common, resulting from deposition of hemoglobin in renal tubules and decreased blood flow. Other complications include non-cardiogenic pulmonary edema, hypoglycemia from hepatic dysfunction, acidosis, anemia, thrombocytopenia, and jaundice. Chronic complications include tropical splenomegaly and quartan malarial nephropathy.
History and examination in orthopedics
History and examination in orthopedicsSalar Jakhsi Orthopedic surgeons deal with diseases and injuries of the musculoskeletal system. Diagnosis depends on taking a thorough history, conducting a physical examination, and ordering investigations. The history focuses on personal details, chief complaints, present illness, past medical history, medications, family history, and social history. The physical examination involves inspecting, feeling, and moving the affected area as well as conducting neurovascular and special tests. Imaging studies like x-rays, CT scans, MRIs, and scans are important investigations to diagnose orthopedic conditions.
Andere mochten auch (6)
Competition Journal Article by Emilio Varanini and Feng Jiang
Competition Journal Article by Emilio Varanini and Feng JiangEmilio Varanini This document summarizes a 2014 Chinese Supreme Court decision regarding antitrust law between Qihoo and Tencent. It discusses how the decision demonstrates China's commitment to developing the rule of law in several ways:
1) By thoroughly applying legal principles and economic theories to complex factual circumstances, helping to balance administrable rules with economic analysis.
2) By establishing an important precedent that lower courts can apply to similar cases, developing China's system of case law.
3) By following due process and protecting the legitimate interests of litigants.
The document argues this decision shows the Chinese judiciary is capable of carrying out the tasks necessary for the rule of law, and its influence will depend on how
Esei masy agraria belanda
Esei masy agraria belandaMargaret Denny Masyarakat agraria di Belanda pada abad ke-16 hingga ke-17 ditandai dengan kegiatan pertanian dan penternakan, yang meningkat akibat revolusi pertanian dan teknologi baru seperti kincir angin. Mereka terkenal dengan pengeluaran tanaman bijirin, industri tekstil, dan penangkapan ikan, serta menjadi pusat utama penternakan lembu tenusu. Ekonomi Belanda mencapai puncak pada abad ke-17, tetapi mulai mengalami kemerosotan pada awal abad ke-18 disebabkan persaingan internasional.
Cdr Harish Pillai Nm
Cdr Harish Pillai Nmhkpillai CDR HARISH PILLAI has over 22 years of experience in various fields including power generation, telecommunications, human resources, and training. He has extensive experience in project management and technical skills. He holds qualifications in electrical engineering, management studies, and signal intelligence. His career skills include business management, technical expertise, leadership, communication, and training. He is suited for roles such as project manager, engineering manager, and technical consultant.
презентация пда на конференцию 27 05 2016
презентация пда на конференцию 27 05 2016Михаил Голубков Документ содержит информацию о всероссийском банковском форуме, посвященном вопросам управления проблемными кредитами и реструктуризации долговых обязательств. Рассматривается деятельность зао 'первое долговое агентство', которое специализируется на урегулировании долгов и управлении задолженностями на сумму более 30 млрд. рублей. Также описаны основные риски кредиторов и механизмы защиты их интересов в процедурах банкротства.
Suresh Sadasivan_SD
Suresh Sadasivan_SDSuresh Sadasivan Suresh Sadasivan is a senior SAP consultant with over 16 years of experience implementing and supporting SAP SD, MM, and EDI modules. He has extensive experience leading implementation projects for various industries including high tech, manufacturing, food and beverage, and public sector. Some of his responsibilities have included managing requirement gathering, blueprinting, configuration, testing, go-live preparation and support.
chandru server_resume
chandru server_resumeChandrasekaran K Chandra Sekaran is a VMware and Windows administrator seeking a career where he can fully utilize his 6+ years of experience in system administration and customer relationship management. He has worked in various roles supporting Windows and VMware environments, including his current role at Solarwinds where he manages a large Windows server infrastructure and virtual environment. He has strong technical skills including VMware, Windows server, Active Directory, and networking fundamentals.
Anzeige
Ähnlich wie buruli ulcer (20)
Buruli ulcer leaflet prin...
Buruli ulcer leaflet prin...Idris Ahmed This document summarizes information about Buruli ulcer, a chronic skin disease caused by Mycobacterium ulcerans. It describes the typical presentation as painless skin lesions that slowly ulcerate. Peak incidence is in children ages 5-15 in central and western Africa near slow-moving bodies of water. While the mode of transmission is unknown, water bugs and fish are believed to carry the bacteria. Treatment involves antibiotics like rifampicin and streptomycin or clarithromycin, with surgery reserved for advanced cases to prevent deformities from scarring.
Buruli ulcer by Dr Earnest Njih Tabah
Buruli ulcer by Dr Earnest Njih TabahEarnestTabah This document provides an overview of Buruli ulcer (BU), a disease caused by Mycobacterium ulcerans. It discusses the definition of BU, historical cases in Cameroon, epidemiology, pathogenesis, diagnosis, management including treatment and wound care, prevention of disability, and organization of BU control in Cameroon. Key points include that BU causes large skin ulcers and tissue destruction if untreated, with over 5 million people at risk in Cameroon. Management involves antibiotic treatment, wound care including cleaning and dressing, and sometimes surgery. Prevention of disability focuses on education, early detection and treatment, wound and joint care, and rehabilitation. BU control in Cameroon is organized at central, regional, and district levels through
infectious diseases
infectious diseasesAndrea B. This document provides information about various staining techniques used in microbiology and pathology. Periodic acid-Schiff staining is used to demonstrate glycogen by oxidizing tissue sections with periodic acid to form aldehyde groups, which are then detected by Schiff reagent to produce a colored product. Mucicarmine staining can also aid in identifying Cryptococcus neoformans fungus due to its mucin capsule staining. Ziehl-Neelsen staining uses an acid-fast dye to identify acid-fast organisms like Mycobacterium tuberculosis.
Cutaneous Antrax & Its Mimics
Cutaneous Antrax & Its MimicsLouie Ray The document provides a differential diagnosis for various ulcerative and eschar-forming skin lesions. It describes the key clinical features of cutaneous anthrax including a painless ulcer covered by a black eschar surrounded by disproportionate edema. Cutaneous leishmaniasis presents as a slowly evolving papule to ulcerative lesion with possible lymphangitis. Cat-scratch disease causes regional lymphadenopathy after a papule or vesicle at the inoculation site.
ATYPICAL MYCOBACTERIAL INFECTIONS AND THEIR MANIFESTATIONS
ATYPICAL MYCOBACTERIAL INFECTIONS AND THEIR MANIFESTATIONSDR. MOHNISH SEKAR The document discusses atypical mycobacterial infections, focusing on non-tuberculous mycobacteria (NTM) such as Mycobacterium kansasii, Mycobacterium marinum, Mycobacterium ulcerans, and Mycobacterium avium complex, including their transmission modes, clinical presentations, and treatment options. While these infections can affect both immunocompromised and healthy individuals, their diagnosis and management can vary significantly depending on the species and severity of the disease. The increasing incidence of these infections, especially among people with weakened immune systems, highlights the importance of awareness and timely intervention.
Mycobacterium ulcerans Methods and Protocols 1st Edition Gerd Pluschke Kathar...
Mycobacterium ulcerans Methods and Protocols 1st Edition Gerd Pluschke Kathar...tresnalockie Mycobacterium ulcerans Methods and Protocols 1st Edition Gerd Pluschke Katharina Röltgen
Mycobacterium ulcerans Methods and Protocols 1st Edition Gerd Pluschke Katharina Röltgen
Mycobacterium ulcerans Methods and Protocols 1st Edition Gerd Pluschke Katharina Röltgen
Communicable disease Pharm. D II Year
Communicable disease Pharm. D II YearImmanuel Jebastine M This document defines and describes several communicable diseases including their symptoms and modes of transmission. Tuberculosis is a bacterial infection of the lungs that spreads through the air when infected individuals cough or sneeze. Symptoms include chronic cough, fever, night sweats and weight loss. Hepatitis is an inflammation of the liver that causes jaundice, fatigue and abdominal pain. It spreads through contact with infected blood or bodily fluids. Malaria is a parasitic infection spread by mosquitos that causes fever, chills and flu-like symptoms.
BURULI ULCER.pptx, MEDICAL MICROBIOLOGY.
BURULI ULCER.pptx, MEDICAL MICROBIOLOGY.AnushaBalakrishnan5 Buruli ulcer is a devastating skin disease caused by the bacterium Mycobacterium ulcerans, primarily affecting individuals near river sides in Africa and Australia. The infection results in severe skin and soft tissue damage, leading to disfigurement and disability, with transmission still largely unknown. Treatment involves antibiotics and possibly surgery, while prevention focuses on early diagnosis, hygiene, and proper wound care.
Leishmaniasis
LeishmaniasisVasyl Sorokhan Leishmaniasis is a parasitic disease spread by sand fly bites. It exists in three main forms: cutaneous, mucocutaneous, and visceral. Cutaneous lesions cause skin sores, while mucocutaneous lesions affect mucosal tissues and can cause disfigurement. Visceral leishmaniasis affects internal organs and is the most serious form. The disease is diagnosed by microscopic examination of tissues or cultures to view the parasites. Treatment depends on the form but may include topical or systemic antimonials, amphotericin B, or miltefosine.
Ulcerative, Vesicular and Bullous Lesions.pptx
Ulcerative, Vesicular and Bullous Lesions.pptxManuelKituzi Ulcerative, vesicular and bullous lesions can be caused by a variety of factors including infection, trauma, allergy and systemic disorders. Herpes simplex virus is a common cause of viral infections presenting as ulcers in the mouth. Primary herpes simplex infection, also known as acute herpetic gingivo-stomatitis, presents with fever and malaise followed by the development of small vesicles that rupture leaving shallow ulcers around 2-6mm in size, often affecting the palate, gums and tongue. The document describes the clinical features and management of various ulcerative conditions of the mouth.
Spillover Animal Infections And The Next Human Pandemic David Quammen
Spillover Animal Infections And The Next Human Pandemic David Quammenkavirareasa9 Spillover Animal Infections And The Next Human Pandemic David Quammen
Spillover Animal Infections And The Next Human Pandemic David Quammen
Spillover Animal Infections And The Next Human Pandemic David Quammen
My project - rate of leprosy infection
My project - rate of leprosy infectionYusuf AbdulGaniyu The document provides background information on leprosy (Hansen's disease), including that it is caused by the bacteria Mycobacterium leprae. It then summarizes the aims and objectives of the study, which are to examine and forecast leprosy prevalence rates in Nigeria between 2005-2014 using time series analysis, and to analyze age and gender distributions of reported cases. The methodology section outlines that secondary data on 474 leprosy cases from a Nigerian medical center over this period will be analyzed using descriptive statistics and time series analysis in MINITAB and Excel to identify trends and patterns in incidence.
Leprosy
Leprosyselva711 Leprosy, also known as Hansen's disease, is a chronic infectious disease caused by Mycobacterium leprae. It primarily affects the skin and peripheral nerves. While leprosy has been associated with stigma, it is generally not very contagious and multi-drug therapy can cure the disease and prevent disability. Leprosy remains endemic in some developing countries, especially India, Brazil, and several countries in Africa and Asia. Early detection and treatment are important to prevent nerve damage and physical disability.
Angyiereyiri_et_al
Angyiereyiri_et_alElijah Dakorah Angyiereyiri This document discusses a study that assessed the impact of mass drug administration (MDA) on the transmission of lymphatic filariasis in Tono Irrigation Area in Navrongo, Ghana. The study involved collecting and dissecting mosquitoes from two communities to determine infection levels. A total of 3,650 Anopheles mosquitoes and 386 Culex mosquitoes were collected and examined. Only 3 Anopheles mosquitoes were found to be infected with filarial parasites, but no infective L3 stage larvae were detected. This suggests that ongoing transmission of lymphatic filariasis had been interrupted in the study sites following over nine years of MDA, though continued surveillance is still needed.
Filariioses 10
Filariioses 10Jasmine John Filarial worms infect over 140 million people worldwide and are transmitted by mosquitoes. They reside in lymphatic vessels and tissues. The most common forms that cause disease are Wuchereria bancrofti, Brugia malayi, Onchocerca volvulus, and Loa loa. They have complex lifecycles involving microfilariae that develop in mosquitoes before infecting humans. Lymphatic filariasis causes lymphatic damage and symptoms like hydrocele, lymphedema, and elephantiasis due to adult worms residing in lymphatics. Treatment involves diethylcarbamazine to kill microfilariae.
Leprosy in Nkhotakota
Leprosy in NkhotakotaHumphrey Misiri This study analyzed records of leprosy cases from Nkhotakota District Hospital in Malawi between 1992-2001:
- A total of 526 leprosy cases were identified, with prevalence rates peaking at 3.39 per 10,000 people in 1995 before declining.
- Paucibacillary leprosy was more common than multibacillary leprosy, accounting for 84.8% of cases.
- More males had multibacillary leprosy compared to females, while more females had paucibacillary leprosy than males.
- The results indicate that paucibacillary leprosy remains a public health issue in the region as a reflection
Tuberculosis
TuberculosisPREJITH AYLARA Tuberculosis (TB) is a bacterial infection that usually affects the lungs. It is caused by Mycobacterium tuberculosis bacteria and spreads through the air. While most people exposed to TB do not develop active symptoms, those with weakened immune systems are at higher risk. Left untreated, active TB can be fatal. Diagnosis involves tests on body fluids and tissues. Treatment requires taking multiple antibiotics for a long period of time. While once common, TB was reduced by antibiotics but has resurfaced in drug-resistant forms, creating a public health crisis in some areas.
Porn Tube Land
Porn Tube Landporntubeland Tropical diseases remain a critical global health issue, particularly in developing countries, where poverty and lack of sanitation exacerbate the problem. Diseases such as malaria, schistosomiasis, and leprosy continue to affect millions, with malaria alone claiming approximately one hundred million lives annually. The World Health Organization's efforts to immunize children against common diseases face challenges due to environmental factors and the increasing spread of diseases through air travel, highlighting the urgent need for more research and effective interventions.
Narh_CA_&_coll_md_2014
Narh_CA_&_coll_md_2014zeiaphil91 The article discusses genotyping tools for differentiating Mycobacterium ulcerans strains, the bacterium responsible for Buruli ulcer, a neglected endemic disease affecting numerous countries. It highlights the importance of molecular epidemiology in tracking infection sources and proposes improvements to existing diagnostic methods to enhance public health efforts against the disease. The authors also call attention to the need for more robust genotyping techniques and the potential advantages of new methods like LAMP over traditional PCR in resource-limited settings.
Bacterial, Viral & Mycotic Infections
Bacterial, Viral & Mycotic Infectionsguest018923 The document provides information on various bacterial, viral, and fungal infections that can affect humans. It discusses specific infections such as actinomycosis, syphilis, tuberculosis, candidiasis, herpes simplex virus, and more. For each infection, it describes the causative agent, transmission, clinical features, histological features, and in some cases treatment. The document is an informative reference for various microbial infections.
Anzeige
buruli ulcer
- 1. GPSA Health Committee Buruli Ulcer What do you know about Buruli ulcer? October, 2014 History and Epidemiology Be informed…. pg. 3 Maecenus quis lacus? Buruli ulcer is a disease of skin and soft tissue with the potential to leave sufferers scarred and disabled. It is caused by an environmental pathogen, Mycobacterium ulcerans, which produces a destructive toxin. The exact mode of transmission is unclear. The main burden of disease falls on children living in sub-Saharan Africa, but healthy people of all ages, races, and socioeconomic classes are susceptible. M. ulcerans is the third most common mycobacterial pathogen of humans, after M. tuberculosis and M. leprae (which cause tuberculosis and leprosy, respectively). The definitive description of M. ulcerans was published in 1948, when MacCallum and others in Australia reported six cases of an unusual skin infection caused by a mycobacterium that could only be cultured when the incubation temperature was set lower than for M. tuberculosis. In Africa, large ulcers almost certainly caused by M. ulcerans had been described by Sir Albert Cook in 1897 and by Kleinschmidt in northeast Congo during the 1920s. The main burden of disease falls on children living in sub- Saharan Africa. Prior to the 1980s, foci of M. ulcerans infection were reported in several countries in sub-Saharan Africa including Congo, Uganda, Gabon, Nigeria, Cameroon, and Ghana. The Uganda Buruli Group coined the name “Buruli ulcer” because the cases they described were first detected in Buruli County, near Lake Kyoga.
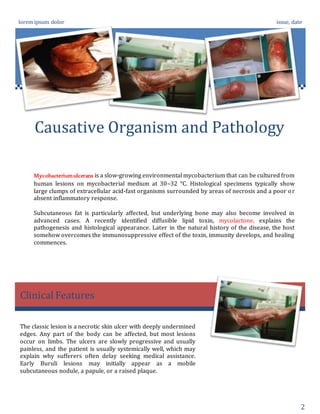
- 2. lorem ipsum dolor issue, date 2 Causative Organism and Pathology Clinical Features Mycobacteriumulcerans is a slow-growing environmental mycobacterium that can be cultured from human lesions on mycobacterial medium at 30–32 °C. Histological specimens typically show large clumps of extracellular acid-fast organisms surrounded by areas of necrosis and a poor or absent inflammatory response. Subcutaneous fat is particularly affected, but underlying bone may also become involved in advanced cases. A recently identified diffusible lipid toxin, mycolactone, explains the pathogenesis and histological appearance. Later in the natural history of the disease, the host somehow overcomes the immunosuppressive effect of the toxin, immunity develops, and healing commences. The classic lesion is a necrotic skin ulcer with deeply undermined edges. Any part of the body can be affected, but most lesions occur on limbs. The ulcers are slowly progressive and usually painless, and the patient is usually systemically well, which may explain why sufferers often delay seeking medical assistance. Early Buruli lesions may initially appear as a mobile subcutaneous nodule, a papule, or a raised plaque.
- 3. lorem ipsum dolor issue, date 3 Future Directions and the End of Obscurity Since 2005, three (3) Buruli Ulcer training workshops have been held in the hospital at which surgical teams in various endemic regions in Ghana are trained Buruli Ulcer Disease has been prevalent in the Asante Akim North District of Ghana since the early 1970s, long before the disease became endemic in the country and the West African Sub Region in the early 1990s. Initially the disease was limited Villages in the Afram Plains sector of the district but it gradually spread to other towns in the district. The Agogo Presbyterian Hospital has been in the forefront of Buruli Ulcer management since the early 1970s. Since 2005, 3 Buruli Ulcer training workshops have been held in the hospital at which surgical teams in various endemic regions in Ghana are trained. In May, 2006, the WHO and the Ministry of Health of Ghana organized an International training workshop on Buruli Ulcer in Agogo Hospital. Participants were drown from all over Africa while the facilitators came from Australia, Switzerland, France, USA, Ghana and Cote D'Ivoire. Due to the efforts of the Buruli Ulcer Volunteers and the Public Health Unit of the hospital an increasing number of nodules and other clinical forms are being identified and brought to the hospital. Buruli Ulcer accounts for about 0.6% of total admissions per year and the average length of stay in hospital is about 90 days. A lot of research into Buruli Ulcer has been carried out in the Agogo Presbyterian Hospital, the latest being a drug trial using Streptomycin and Rifampicin as well as Clarithromycin and Rifampicin. Buruli ulcer is now emerging from long years of neglect: interest and momentum are growing. However, there is much to do if we are to understand why the disease is becoming more common and how this relates to human activity. The current control strategy of early detection and treatment should be scaled up in the affected countries. Our ultimate goal is the development of an effectiveand safe vaccine able to provide long-lasting protection for those who live in endemic areas. The Research and Information Team (Health Committee)
- 4. lorem ipsum dolor issue, date 4 Continued Why Has Buruli Ulcer Been Neglected Until Now? A subgroup of patients present with rapidly progressive oedema of a whole limb, abdominal wall, or side of the face without an obvious focal lesion. Part or all of the affected area will subsequently ulcerate, although anecdotal reports suggest that timely antibiotic therapy may greatly reduce the resulting necrosis. "They call it the mysterious disease because nobody knows how it's transmitted," said Fogarty grantee Dr. Richard W. Merritt, of Michigan State University. "If you ask, what do you think causes it, you get a variety of answers. It's a tough one." Case control studies have suggested that farming activities close to rivers in endemic areas are a risk factor for Buruli ulcer, but for farmers involved in subsistence agriculture, avoidance of riverine areas is difficult. A recent study from Ghana has suggested that swimming in rivers may also be an independent risk factor. To date, the main focus of public health efforts has been on early detection and treatment, which greatly reduce morbidity and cost. Despite its long history, Buruli ulcer has gone largely unnoticed until recently. Buruli ulcer typically occurs in poor rural communities with little economic or political influence. Rural isolation may mean that national surveillance systems do not immediately detect the appearance of new outbreaks. Affected populations may believe that there is no effective medical treatment for the disease, which discourages them from seeking assistance. In the developed world, Buruli ulcer is frequently omitted from standard medical texts and undergraduate medical courses. The absence of a potentially profitable market has meant that there has been little private investment to date in drug and vaccine development or in research to improve prospects for better control.