Filter
2643
Text search:
national
tuberculosis
Programme
Featured
289
807
Language
2439
139
57
46
16
14
9
8
4
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Document type
1525
458
336
134
111
30
21
16
5
2
1
1
Countries
178
111
84
80
71
64
63
58
56
55
50
48
48
48
46
40
38
38
37
28
27
24
22
22
21
21
20
18
17
15
14
14
13
12
11
11
11
10
9
9
9
9
8
7
7
7
6
6
5
5
5
5
5
5
5
4
4
4
4
4
4
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
412
157
78
75
70
65
46
43
37
28
24
24
21
20
18
18
16
16
16
15
15
14
13
12
12
12
12
11
11
10
10
10
10
10
9
9
9
9
9
9
8
8
8
8
8
7
7
7
7
7
7
7
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Publication Years
703
1669
258
13
Category
1193
196
154
101
100
40
29
Toolboxes
472
184
106
103
77
68
62
58
53
46
45
43
42
39
33
33
30
29
26
17
17
3
3
2
1
1

The Regional Action Framework for Noncommunicable Disease Prevention and Control provides a unified vision of objectives and recommended actions to combat the noncommunicable disease (NCD) epidemic in the Western Pacific Region. Implementation should be supported by cross-sectoral coordination
...
, sustainable financing, evidence-based policy, and community engagement, tailored to each Member State’s unique context. In doing so, Member States are encouraged to transform a disease treatment-centered “sick system” into a “health system” in which a population’s health and well-being enable socioeconomic development.
more

Global Vaccine Summit 2020 - Chair’s Summary
Global Alliance for Vaccines and Immunisation (Gavi)
Global Alliance for Vaccines and Immunisation (Gavi)
(2020)
CC
The UK government hosted the Global Vaccine Summit on June 4, 2020 under the patronage of the Rt. Hon. Boris Johnson, Prime Minister of the United Kingdom of Great Britain and Northern Ireland. The meeting was held by videoconference in light of the ongoing COVID-19 pandemic. 2. The Summit brought
...
together more than 300 people, including 42 Heads of State and Government. 62 countries were represented, notably 14 Gavi implementing countries, all of the G7 nations and 19 governments of the G20. Eminent participants also included H.E. Antonio Guterres, Secretary-General of the United Nations; H.E. Moussa Faki Mahamat, Chairperson of the African Union Commission; H.E. Dr Tedros Adhanom Ghebreyesus, WHO Director-General; H.E. Henrietta Fore, UNICEF Executive Director; Bill Gates, Co-Chair of the Bill & Melinda Gates Foundation; Ministers from implementing and donor countries; CEOs of vaccine manufacturing companies and private sector partners; leaders of UN and other international agencies; senior civil society representatives; and Gavi champions. A full list of the participants can be found in Annex.
more

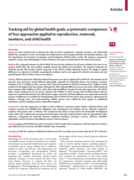
There has been no systematic comparison of how the policy response to past infectious disease outbreaks and epidemics was funded. This study aims to collate and analyse funding for the Ebola epidemic and Zika outbreak between 2014 and 2019 in order to understand the shortcomings in funding reporting
...
and suggest improvements. Methods: Data were collected via a literature review and analysis of financial reporting databases, including both amounts donated and received. Funding information from three financial databases was analysed: Institute of Health Metrics and Evaluation’s Development Assistance for Health database, the Georgetown Infectious Disease Atlas and the United Nations Financial Tracking Service. A systematic literature search strategy was devised and applied to seven databases: MEDLINE, EMBASE, HMIC, Global Health, Scopus, Web of Science and EconLit. Funding information was extracted from articles meeting the eligibility criteria and measures were taken to avoid double counting. Funding was collated, then amounts and purposes were compared within, and between, data sources.
more

I examine the effectiveness of donors in targeting the highest burden of malaria in the Democratic Republic of Congo when health information structure is fragmented. I exploit local variations in the burden of malaria induced by mining activities as well as financial and epidemiological data from he
...
alth facilities to estimate how local aid is matching local health needs. Using a regression discontinuity design, I find significant but quantitatively small variations in aid to health facilities located within mining areas. Comparing local aid with the additional cost of treatment and prevention associated with the increased risk of malaria transmission, I find suggestive evidence that local populations with the highest burden of the disease receive a proportionately lower share of aid compared to neighbouring areas with reduced exposure to malaria infection. The evidence of disparities in the allocation of aid for malaria supports the view that donors may have inaccurate information about local population needs.
more

Over the 20 years that followed, this unique partnership has invested more than US$53 billion, saving 44 million lives and reducing the combined death rate from the three diseases by more than half in the countries in which the Global Fund invests.
Four initiatives have estimated the value of aid for reproductive, maternal, newborn, and child health
(RMNCH): Countdown to 2015, the Institute for Health Metrics and Evaluation (IHME), the Muskoka Initiative, and
the Organisation for Economic Co-operation and Development (OECD) policy marker. We
...
aimed to compare the
estimates, trends, and methodologies of these initiatives and make recommendations for future aid tracking.
more

Heart failure with a reduced ejection fraction (HFrEF) is a condition frequently encountered by healthcare professionals and, in order to achieve the best outcomes for patients, needs to be managed optimally. This guideline document is based on the European Society of Cardiology Guidelines for the t
...
reatment of acute and chronic heart failure published in 2016, and summarises what is considered the best current management of patients with the condition. It provides information on the definition, diagnosis and epidemiology of HFrEF in the African context. The best evidence-based treatments for HFrEF are discussed, including established therapies (beta-blockers, ACE-i/ARBs, mineralocorticoid receptor antagonists (MRAs), diuretics) that form the cornerstone of heart failure management as well as therapies that have only recently entered clinical use (angiotensin receptor-neprilysin inhibitor (ARNI), sodium/glucose cotransporter-2 (SGLT2) inhibitors). Guidance is offered in terms of more invasive therapies (revascularisation, implantable cardioverter defibrillators (ICDs) and cardiac resynchronisation therapy (CRT) by implantation of a biventricular pacemaker with (CRT-D) or without (CRT-P) an ICD, left ventricular assist device (LVAD) use and heart transplantation) in order to ensure efficient use of these expensive treatment modalities in a resourcelimited environment. Furthermore, additional therapies (digoxin, hydralazine and nitrates, ivabradine, iron supplementation) are discussed and advice is provided on general preventive strategies (vaccinations). Sections to discuss conditions that are particularly prevalent in sub-Saharan Africa (HIV-associated cardiomyopathy (CMO), peripartum CMO, rheumatic heart disease, atrial fibrillation) have been added to further improve clinical care for these commonly encountered disease processes.
more
The World Heart Federation (WHF) Roadmap series covers a large range of cardiovascular conditions. These Roadmaps identify potential roadblocks and their solutions to improve the prevention, detection and management of cardiovascular diseases and provide a generic global framework available for loca
...
l adaptation. A first Roadmap on raised blood pressure was published in 2015. Since then, advances in hypertension have included the publication of new clinical guidelines (AHA/ACC; ESC; ESH/ISH); the launch of the WHO Global HEARTS Initiative in 2016 and the associated Resolve to Save Lives (RTSL) initiative in 2017; the inclusion of single-pill combinations on the WHO Essential
Medicines’ list as well as various advances in technology, in particular telemedicine and mobile health. Given the substantial benefit accrued from effective interventions in the management of hypertension and their potential for scalability in low and middle-income countries (LMICs), the WHF has now revisited and updated the ‘Roadmap for raised BP’ as ‘Roadmap for hypertension’
by incorporating new developments in science and policy. Even though cost-effective lifestyle and medical interventions to prevent and manage hypertension exist, uptake is still low, particularly in resource-poor areas. This Roadmap examined the roadblocks pertaining to both the demand side (demographic and socio-economic factors, knowledge and beliefs, social relations, norms, and
traditions) and the supply side (health systems resources and processes) along the patient pathway to propose a range of possible solutions to overcoming them. Those include the development of population-wide prevention and control programmes; the implementation of opportunistic screening and of out-of-office blood pressure measurements; the strengthening of primary care and a greater focus on task sharing and team-based care; the delivery of people-centred care and stronger patient and carer education; and the facilitation of adherence to treatment. All of the above are dependent upon the availability and effective distribution of good quality, evidencebased, inexpensive BP-lowering agents.
more
Cholera is an acute gastrointestinal infection caused by the bacterium Vibrio Cholerae serogroup O1 or O139, and is often linked to unsafe drinking water, lack of proper sanitation and personal hygiene. It adversely affects mostly the poor and vulnerable populations in countries, which are already d
...
eprived of proper health facilities and conducive environmental conditions. The disease spreads through oro-fecal transmission by the ingestion of contaminated food or water or by person-to-person contact. It has a short incubation period of 2 hours to 5 days and the number of affected cases can rapidly increase across large regions. Cholera is a significant threat to global public health leading to an estimated 3-5 million cases per year worldwide, with an annual toll of 100,000 deaths. The disease was first reported in 1817 from the Ganges Delta of India and since then the ongoing 7th pandemic has emerged from Indonesia, reached Africa in 1970 and Somalia happens to be one of the early affected countries. Over the past few decades,
Somalia has witnessed the occurrence of repeated AWD/Cholera disease outbreaks that have caused high morbidity and mortality across the country.
more

Introduction Community health workers (CHWs) are increasingly being tasked to prevent and manage cardiovascular disease (CVD) and its risk factors in underserved populations in low-income and middle-income countries (LMICs); however, little is known about the required training necessary for them to
...
accomplish their role. This review aimed to evaluate the training of CHWs for the prevention and management of CVD and its risk factors in LMICs.
Methods A search strategy was developed in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, and five electronic databases (Medline, Global Health, ERIC, EMBASE and CINAHL) were searched to identify peer-reviewed studies published until December 2016 on the training of CHWs for prevention or control of CVD and its risk factors in LMICs. Study characteristics were extracted using a Microsoft Excel spreadsheet and quality assessed using Effective Public Health Practice Project’s Quality Assessment Tool. The search, data extraction and quality assessment were performed independently by two researchers.
Results The search generated 928 articles of which 8 were included in the review. One study was a randomised controlled trial, while the remaining were before–after intervention studies. The training methods included classroom lectures, interactive lessons, e-learning and online support and group discussions or a mix of two or more. All the studies showed improved knowledge level post-training, and two studies demonstrated knowledge retention 6 months after the intervention.
Conclusion The results of the eight included studies suggest that CHWs can be trained effectively for CVD prevention and management. However, the effectiveness of CHW trainings would likely vary depending on context given the differences between studies (eg, CHW demographics, settings and training programmes) and the weak quality of six of the eight studies. Well-conducted mixed-methods studies are needed to provide reliable evidence about the effectiveness and cost-effectiveness of training programmes for CHWs.
more
Alcohol consumption is deeply embedded in the social landscape of many societies. Several major factors have an impact on levels and patterns of alcohol consumption in populations – such as historical trends in alcohol consumption, the availability of alcohol, culture, economic status and trends i
...
n the marketing of alcoholic beverages, as well as implemented alcohol control measures. At the individual level, the patterns and levels of alcohol consumption are determined by many different factors, including gender, age and individual biological and socioeconomic vulnerability factors, as well as the policy environment. Prevailing social norms that support drinking behaviour and mixed messages about the harms and benefits of drinking encourage alcohol consumption delay appropriate health-seeking behaviour and weaken community action
more

People with disabilities experience significant health inequalities. In Malawi, where most individuals live in low-income rural settings, many of these inequalities are exacerbated by restricted access to health care services. This qualitative study explores the barriers to health care access experi
...
enced by individuals with a mobility or sensory impairment, or both, living in rural villages in Dowa district, central Malawi. In addition, the impact of a chronic lung condition, alongside a mobility or sensory impairment, on health care accessibility is explored.
more
Noncommunicable diseases (NCDs) – chief among them, cardiovascular diseases (heart disease and stroke), cancer, diabetes and chronic respiratory diseases – along with mental health, cause nearly three quarters of deaths in the world. Their drivers are social, environmental, commercial and geneti
...
c, and their presence is global. Every year 17 million people under the age of 70 die of NCDs, and 86% of them live in low- and middle-income countries (LMICs).
more
Noncommunicable diseases (NCDs) – chief among them, cardiovascular diseases (heart disease and stroke), cancer, diabetes and chronic respiratory diseases – along with mental health, cause nearly three quarters of deaths in the world. Their drivers are social, environmental, commercial and geneti
...
c, and their presence is global. Every year 17 million people under the age of 70 die of NCDs, and 86% of them live in low- and middle-income countries (LMICs).
more

Risk factors for asthma among schoolchildren who participated in a casecontrol study in urban Uganda
Data on asthma aetiology in Africa are scarce. We investigated the risk factors for asthma among schoolchildren (5–17 years) in urban Uganda. We conducted a case-control study, among 555 cases and 1115 controls. Asthma was diagnosed by study clinicians. The main risk factors for asthma were tertia
...
ry education for fathers (adjusted OR (95% CI); 2.32 (1.71–3.16)) and mothers (1.85 (1.38–2.48)); area of residence at birth, with children born in a small town or in the city having an increased asthma risk compared to schoolchildren born in rural areas (2.16 (1.60–2.92)) and (2.79 (1.79–4.35)), respectively; father’s and mother’s history of asthma; children’s own allergic conditions; atopy; and cooking on gas/electricity. In conclusion, asthma was associated with a strong rural-town-city risk gradient, higher parental socio-economic status and urbanicity. This work provides the basis for future studies to identify specific environmental/lifestyle factors responsible for increasing asthma risk among children in urban areas in LMICs.
more

The global prevalence, morbidity and mortality related to childhood asthma among children has increased significantly over the last 40 years. Although asthma is recognized as the most common chronic disease in children, issues of underdiagnosis and undertreatment persist. There are substantial globa
...
l variations in the prevalence of asthma symptoms in children, with up to 13-fold differences between countries. The rising number of hospital admissions for asthma may reflect an increase in asthma severity, poor disease management and/or the effect of poverty. The financial burden of asthma is relatively high within developed countries (those for which data is available) spending 1 to 2% of their healthcare budget on this condition. Established in 1989, the Global Initiative for Asthma (GINA) attempts to raise awareness about the increasing prevalence of asthma, improve management and reduce the burden of asthma worldwide. Despite global efforts, GINA has not achieved its goal, even among developed nations. There are multiple barriers to reducing the global burden of asthma, including limited access to care and/or medications, and lack of prioritization as a public healthcare priority. In addition, the diversity of healthcare systems worldwide and large differences in access to care require that asthma management guidelines be tailored to local needs.
more

This document provides a list of key WHO-recommended maternal and newborn health commodities and aims to accelerate progress towards the SDGs. It consolidates the key and enabling commodities from existing WHO guidelines on maternal and newborn health.

The South African WHO Country Cooperation Strategy (CCS) 2023–2027 focuses on four key strategic priorities based on the country’s health needs and disease epidemiology, while also considering the need for building resilient health systems for UHC and health security in the post pandemic period.
...
These include:
1. augment health systems strengthening reforms to accelerate progress towards universal health coverage.
2. address the quadruple burden of diseases and promote well-being across the life course in view of achieving global targets.
3. build health systems resilience and strengthen health emergency preparedness and response capacities.
4. enhance multisectoral collaboration and global partnerships for concerted action on health and its determinants.
In order to harness its expertise across its three levels, namely: the WHO Country Office (WCO), WHO Regional Office for Africa, and WHO headquarters, WHO will work closely and collaboratively with the Government of South Africa to implement the 2023–2027 strategic priorities.
more

Guidelines approved by the WHO Guidelines -Review Committee; second edition

PLoS ONE 18(5): e0285031. https://doi.org/10.1371/journal.pone.0285031
The study aims to integrate HPV vaccination into routine care in adolescent HIV clinics. To achieve success, we will co-design a package of implementation strategies using a previously successful implementation research approach
...
developed for cervical cancer prevention in LMICs: the Integrative Systems Praxis for Implementation Research (INSPIRE). INSPIRE is a novel, comprehensive approach to develop, implement, and evaluate implementation science efforts
more