Filter
2295
Filtered Results: 2295
Text search:
H.
Advani
Featured
Recommendations
227
New Publications
455
Language
Document type
No document type
1174
Studies & Reports
515
Guidelines
310
Manuals
131
Strategic & Response Plan
69
Training Material
41
Fact sheets
31
Situation Updates
10
Resource Platforms
7
Infographics
3
Brochures
2
App
1
Online Courses
1
Countries / Regions
India
117
Global
102
Indonesia
58
Kenya
53
South Africa
53
Ethiopia
35
Latin America and the Carribbean
34
Nepal
33
Zambia
32
Africa
31
Western and Central Europe
31
Tanzania
30
Nigeria
26
Malawi
26
Bangladesh
25
Sierra Leone
24
Syria
24
Myanmar / Burma
24
Uganda
23
Liberia
22
Philippines
20
Rwanda
18
Ukraine
17
Namibia
17
Cambodia
15
Ghana
14
Asia
14
Eastern Europe
14
Zimbabwe
13
South–East Asia Region
12
Brazil
12
Russia
12
South Sudan
12
Lesotho
11
Mozambique
11
Congo, Democratic Republic of
11
Senegal
9
Burkina Faso
9
Afghanistan
9
Botswana
9
Cameroon
8
Guinea
8
Vietnam
8
Eswatini/ Swaziland
8
Peru
7
USA
7
Germany
7
East and Southern Africa
7
Colombia
6
China
6
Middle East and North Africa
6
Eastern Europe and Central Asia
6
Argentina
6
Yemen
6
Somalia
6
Ecuador
6
Pakistan
6
Laos
5
West and Central Africa
5
Western Pacific Region
5
Lebanon
5
Mali
5
Thailand
4
El Salvador
4
Chile
4
Sudan
4
Iraq
4
Albania
3
Niger
3
Burundi
3
Haiti
3
Venezuela
3
Paraguay
3
North America
3
Sri Lanka
3
Angola
3
Mexico
2
Benin
2
Qatar
2
Jordan
2
Jamaica
2
Japan
2
Spain
2
Israel
2
Bosnia and Herzegovina
2
Côte d’Ivoire / Ivory Coast
2
Greece
2
Georgia
2
Chad
2
Libya
2
Madagascar
2
Tajikistan
1
North Korea
1
Timor Leste/ East Timor
1
Serbia
1
Turkey
1
Gambia
1
Kazakhstan
1
Fiji
1
Kyrgyzstan
1
Congo-Brazzaville
1
Morocco
1
Mauritania
1
Italy
1
Armenia
1
Dominican Republic
1
Guinea-Bissau
1
Saudi Arabia
1
France
1
Mauritius
1
Tunisia
1
United Kingdom
1
Portugal
1
Belarus
1
Bolivia
1
Nicaragua
1
Moldova
1
Egypt
1
Palestine
1
Central African Republic
1
Honduras
1
Bhutan
1
Cuba
1
Guatemala
1
Authors & Publishers
Publication Years
Category
Countries
752
Clinical Guidelines
224
Public Health
142
Key Resources
126
Women & Child Health
118
Capacity Building
45
Pharmacy & Technologies
22
Toolboxes
HIV
180
COVID-19
168
Mental Health
158
TB
135
Planetary Health
123
NTDs
106
Caregiver
99
Disability
80
Global Health Education
54
AMR
50
Conflict
49
Ebola & Marburg
47
NCDs
47
Health Financing Toolbox
45
Pharmacy
37
Rapid Response
35
Refugee
34
Natural Hazards
28
Social Ethics
19
Malaria
19
2.0 Rapid Response
16
Specific Hazards
12
Polio
11
Cholera
6
Zika
6

This Implementation Kit (I-Kit), developed by the Health Communication Capacity Collaborative (HC3), which is funded by USAID and based at the Johns Hopkins Center for Communication Programs, offers structured guidance for improving social and behavioural change communication (SBCC) strategies relat...

The Manual for Parasitological Surveillance in Prevention of Reintroduction or Re-establishment of Malaria in Sri Lanka (2019) provides guidelines to health professionals on how to conduct effective malaria surveillance to prevent the reintroduction of the disease in Sri Lanka, which was certified m...

The project was developed by the International Federation of Medical Students’ Associations (IFMSA), in line with the Federation’s statement “a world in which students are equipped with knowledge, skills and value to take on health leadership roles locally and globally so to...

A aplicação da tecnologia digital de saúde está crescendo rapidamente na África, com o
objetivo de melhorar a prestação de serviços de saúde e alcançar de forma mais eficaz
comunidades remotas e carentes. A falta de diretrizes e padrões habilitadores em todo o
continente, por outro ...
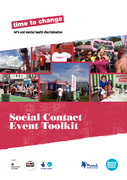
This toolkit will help you to plan and run an event that helps to change the way that people in your community think about, and behave towards, people with mental health problems


Skin and mucosal conditions are extremely common in all children and adults in particular in HIV-infected adults and children and are one of the commonest daily management problems faced by health care workers caring for patients with HIV infection

Frequently asked questions (FAQs)
This document highlights COVID-19 specific considerations in relation to camp and camp-like settings, and is intended to assist in guiding operations where camp/site management5 is being implemented. Although the guidance - structured around questions from the fiel...

For COVID-19, as for many infectious diseases, the true level of transmission is frequently underestimated because a substantial proportion of people with the infection are undetected either because they are asymptomatic or have only mild symptoms and thus typically fail to present at healthcare fac...

Policy
July 2012
Working Paper No. 3

Despite the stated centrality of protection in humanitarian action and a growing attention to protection activities, the evaluation of protection has received relatively little attention. This pilot guide seeks to fill this gap, providing insights and guidance to those evaluating protection in the c...

Comprehensive public health action on population ageing is urgently needed. This will require fundamental shifts, not just in the things we do, but in how we think about ageing itself. The World report on ageing and health outlines a framework for action to foster Healthy Ageing built around the new...

Guide technique pour la prise en charge des maladies cardiovasculaires dans le cadre des soins de santé primaires

Accessed Febr. 6 ,2020

Recommendations to develop guidelines on community-based rehabilitation (CBR) were made during the International Consultation to Review Community-based Rehabilitation which was held in Helsinki, Finland in 2003. WHO; the International Labour Organization; the United Nations Educational, Scientific ...

The occurrence of a high percentage of couterfeit medicines on the global medicines market is often attributed to a lack of effective regulation and a weak enforcement capacity. This review, while focusing on counterfeit medicines and medical devices in developing countries, will present information...

Maternal Child Nutrition. 2017;e12478
This paper analyzes individual level and household level determinants of anemia among children and women in Nepal and Pakistan. Applying multivariate modified Poisson models to recent national survey data, we find that the prevalence of anemia was significa...
This paper analyzes individual level and household level determinants of anemia among children and women in Nepal and Pakistan. Applying multivariate modified Poisson models to recent national survey data, we find that the prevalence of anemia was significa...

WHO today published the new edition of its Model Lists of Essential Medicines and Essential Medicines for Children, which include new treatments for various cancers, insulin analogues and new oral medicines for diabetes, new medicines to assist people who want to stop smoking, and new antimicrobials...

A Manual for Field Staff and Practitioners