Filter
1139
Filtered Results: 1139
Text search:
запор
Featured
Recommendations
74
New Publications
80
Language
English
941
Russian
226
Spanish
152
French
132
Arabic
100
Chinese
68
Portuguese
48
Ukrainian
15
Bengali
9
Swahili
9
Hindi
8
Somali
7
Burmese
7
German
4
Italian
3
Vietnamese
3
Indonesian
3
Japanese
3
Polish
2
Turkish
2
Farsi
2
Afrikaans
1
Bosnian
1
Greek
1
Pashto
1
Georgian
1
Macedonian
1
Zulu
1
Swedish
1
Document type
Studies & Reports
284
No document type
248
Guidelines
200
Fact sheets
110
Strategic & Response Plan
80
Manuals
53
Infographics
47
Resource Platforms
32
Online Courses
19
Training Material
18
Videos
18
Brochures
16
Dashboards/Maps
10
Situation Updates
3
App
1
Countries / Regions
Global
400
Africa
85
Russia
70
Latin America and the Carribbean
33
Ukraine
24
North America
20
Eastern Europe
18
Eastern Europe and Central Asia
17
India
16
Western and Central Europe
15
South Africa
15
South–East Asia Region
13
Asia
12
Middle East and North Africa
7
East and Southern Africa
6
Brazil
6
Germany
5
West and Central Africa
5
Ethiopia
5
Malawi
4
USA
4
Syria
3
Zimbabwe
3
Western Pacific Region
3
Bangladesh
3
Tajikistan
2
Thailand
2
Kenya
2
Ghana
2
Sierra Leone
2
China
2
Nigeria
2
Mozambique
2
Saudi Arabia
2
Congo, Democratic Republic of
2
Angola
2
Somalia
2
Liberia
2
Nepal
1
Turkey
1
Rwanda
1
Albania
1
Singapore
1
Senegal
1
Estonia
1
Kyrgyzstan
1
Burkina Faso
1
Afghanistan
1
Guinea
1
Armenia
1
Guinea-Bissau
1
Tanzania
1
Jamaica
1
United Kingdom
1
Southern Africa
1
Côte d’Ivoire / Ivory Coast
1
Bolivia
1
Barbados
1
United Arab Emirates
1
Vietnam
1
Moldova
1
Namibia
1
Egypt
1
Sudan
1
Yemen
1
Georgia
1
Poland
1
Mali
1
Chad
1
South Sudan
1
Ecuador
1
Bahamas
1
Pakistan
1
Authors & Publishers
World Health Organization WHO
217
World Health Organization (WHO)
97
et al.
72
World Health Organization
54
World Health Organisation (WHO)
26
WHO
21
Pan American Health Organisation PAHO
18
Pan American Health Organization (PAHO)
18
Pan American Health Organization PAHO
17
unicef
13
Всемирная организация здравоохранения (Eвропейское)
12
National Asthma Education Programme
11
American Lung Association
10
Africa CDC Centres for Disease Control and Prevention
8
African Union
8
Center for Disease Control and Prevention CDC
8
Diabetes.co.uk. the global diabetes community
8
Learning about Diabetes, Inc.
8
The Lancet Global Health
8
Всемирная организация здравоохранения (ВОЗ)
8
Allergy Foundation South Africa
7
COPD Foundation
7
United States Agency for International Development (USAID)
7
World Health Organization WHO, et al.
7
International Diabetes Federation
6
United Nations General Assembly
6
United Nations Secretary-General
6
World Health Organization WHO, Regional Office of Europe
6
World Heart Federation
6
Всемирная Организация Здравоохранения
6
Bousquet, J.
5
International Association for Child and Adolescent Psychiatry and Allied Professions
5
National Institute for Communicable Disease (NICE)
5
Open WHO
5
Our World in Data
5
World Bank
5
World Health Organization (WHO), Regional Office for South-East-Asia
5
Youtube
5
ВОЗ
5
Саратовский научно-медицинский журнал
5
Adeloye, D.
4
Africa Center for Disease Control and Prevention
4
COU Family TV
4
Global Initiative for Asthma
4
National Heart, Lung, and Blood Institute
4
National Institute for Health and Care Excellence (NICE)
4
National Library of Medicine
4
Organisation Mondiale de la Santé OMS
4
reliefweb
4
Respiratory Medicine
4
UNAIDS
4
Департамент здравоохранения города Москвы
4
Asher, I.
3
British Heart Foundation
3
Centers for Disease Control and Prevention
3
Centers for Disease Control and Prevention (CDC)
3
Centers for Disease Control and Prevention CDC
3
Chimbari, M.J.
3
Dunn, M.
3
Eastern Mediterranean Region
3
Flood, D.
3
Global Initiative for Chronic Obstructive Lung Disease (GOLD)
3
Global Initiative for Chronic Obstructive Lung Disease – GOLD
3
Journal of Thoracic Disease
3
Levin, M.
3
Mediclinic Southern Africa
3
Médecins Sans Frontières
3
Médecins Sans Frontières (MSF)
3
Ministry of Health Malawi
3
Mortimer, K.
3
NCD Alliance
3
Organisation Mondiale de la Santé OMS, et al.
3
Ritchie, H.
3
Roser, M.
3
Seiglie, J.A.
3
South African Medical Journal
3
The Lancet
3
WHO Africa
3
World Health Organization Africa Region
3
Министерство здравоохранения Российской Федерации
3
Саратовский научно-медицинский журнал.
3
Achieving control of asthma in children in africa - acacia
2
Africa Center for Disease Control and Prevention CDC
2
Africa Region
2
Alan J. Flisher, Michelle Funk, Natalie Drew et al.
2
American College of Cardiology - NCD Academy
2
American Thoracic Society
2
Andrew Moran
2
BMC Medicine
2
BMC Part of Springer Nature
2
BMJ Journals
2
Bulletin of the World Health Organization
2
Bush, A.
2
Calligaro, G.
2
CDC
2
Circulation
2
Corinne Danet, and Florence Fermon
2
Cruz, A.A.
2
de Carvalho-Pinto, R. M.
2
Delfini Cançado, J. E.
2
Diabetes Africa Ltd.
2
Dowse, R.
2
European Centre for Disease Prevention and Control
2
European Centre for disease prevention and control (ECDC)
2
European Centre for Disease Prevention and Control ECDC
2
European Respiratory Journal (ERJ)
2
European Society of Cardiology
2
Frontiers in Cardiovascular Medicine
2
García-Marcos, L.
2
GiZ Deutsche Gesellschaft für Internationale Zusammenarbeit
2
Global Allergy and Airways Patient Platform
2
Global Asthma Network
2
Health Cluster
2
Indian Council of Medical Research
2
Institute for Health Metrics and Evaluation (IHME)
2
International Primary Care - Respiratory Group
2
International Primary Care Respiratory Group (IPCRG)
2
International Union Against Tuberculosis and Lung Disease
2
Juniper, E. F.
2
Khaltaev, N.
2
Kwizera, R.
2
Medscape
2
Menezes Pizzichini, M. M.
2
Ministry of Health Ghana
2
Misereor
2
Mosenifar, Z.
2
NADMO Ghana
2
Nafti, S.
2
National Heart, Lung, and Blood Institute (NHLBI)
2
National Institutes of Health (NIH)
2
Ndlovu, V.
2
npj Primary Care Respiratory Medicine
2
Organisation mondiale de la santé
2
Organisation mondiale de la Santé (OMS)
2
Pan African Thoracic Society
2
Pan American Health Organization
2
Pawankar, R.
2
Reddel, H. K.
2
Regional Office for Africa
2
Robert-Koch-Institut RKI, Deutsches Grünes Kreuz
2
Rodriguez, A.
2
Science Direct
2
Sibanda, E.
2
Sibanda, E.N.
2
Sirinivas, S.
2
Song, P.
2
Sorkness, C. A.
2
The Lancet healthy Longevity
2
U.S. Pharmacist
2
UNODC
2
van Dyk, L.
2
World Health Organization (WHO) Regional Office for the Eastern Mediterranean
2
World Health Organization, Western Pacific Region
2
Wrench, W.
2
ФГБУ «НМИЦ ФПИ»
2
Федеральное государственное бюджетное учреждение «Национальный медицинский исследовательский центр фтизиопульмонологии и инфекционных заболеваний» Министерства здравоохранения Российской Федерации
2
A. Montresor
1
Aarthi, G.R.
1
Abbass, M.M.
1
Abdool-Gaffar, M. S.
1
Abdullah, W.H.
1
Abetz, L.
1
Abubakar, B.K.
1
Acta Scientific Medical Sciences
1
ActionAid, ВОЗ, ЮНИСЕФ, et al.
1
Adachi, Y.
1
adapted from Bang et al., Ann Intern Med (2009)
1
Aday A.W.
1
Aday, A.W.
1
Adcock, I. M.
1
Adhikari, B.
1
Adler, A.J.
1
Africa CDC: Centres for Disease Control and Prevention
1
Africa Centres for Disease Control and Prevention Center for Disease Dynamics, Economics & Policy
1
African Diabetes Education Program
1
African Health Organisation
1
African Journal of Primary Health Care & Family Medicine
1
African Palliative Care Association
1
Afshin, A.
1
Agyemang, C.
1
Ahmad Hassali, M.A.
1
Ahmad, U., Chau, D.M. et al.
1
AI.COMM
1
Aikulola, S.
1
Al Moosawi, S.
1
Al Senany, S.
1
Al-Jawaldeh, A.
1
Al-Otheimin, H. K.
1
Alam, S.
1
Alemayohu, M.A.
1
Alexander Butchart, David Brown, Andrew Wilson, and Christopher Mikton
1
Alexander von Gontard
1
Aliku, T. et al.
1
Alizadeh, M.
1
Allergy: Volume62, Issues84 November 2007 Pages 1-41
1
Allwood, B.
1
Almarzooq, Z.I. et al.
1
Alphonsus, C.
1
Alwan A., McColl K. et al.
1
American Diabetes Association in collaboration with the Centers for Disease Control and Prevention (CDC)
1
American Diabetes Association Professional Practice Committee
1
American Heart Association
1
American Journal of Physiology - Lung Cellular and Molecular Physiology
1
Amini, M.
1
Amnatsatsue, K.
1
Amusa, G.A.
1
Anand, S.
1
Anand, Shuchi
1
and J. Kinyanjui
1
Anderson, L.
1
Annamali, M.
1
Anthonisen, N.R.
1
Arinola, G.O.
1
Armed Forces Pest Management Board, USA
1
Arquivos Brasileiros de Cardiologia
1
Asthma and Lung UK
1
Australian Commission on Safety and Quality in Health Care (ACSQHC)
1
Awokola, B.I.
1
Ärztliches Zentrum für Qualität in der Medizin ÄZQ
1
ÄZQ
1
ÄZQ, BÄK, KBV
1
Baatjies, R.
1
Baert, B.
1
Balcha Hailu, F.
1
Baptist, A.P.
1
Barnes, H.
1
Bartlett, E. S.
1
Basquil, C.
1
Bateman, E. D.
1
Bateman, E.D.
1
Baxter, N.
1
Bayrisches Landesamt für Gesundheit und Lebensmittelsicherheit (LGL)
1
Bazargani, Y.T.
1
BDJ Team
1
Beasley, R.
1
Beauftragte der Bundesregierung für Migration, Flüchtlinge und Integration
1
Becker, A.
1
Begum, T. S. M.
1
Ben Naafs, et al.
1
Benjamin O Alli [et al.]
1
Bertozzi, Stefano
1
Bettercare
1
Bhana, S.
1
BioMed Central
1
Bixby, H.
1
Blanc, P.D.
1
Blanco, I.
1
Bloom, Barry R.
1
BMC
1
BMC Cardiovascular Disorders
1
BMC Health Services Research, part of Springer Nature
1
BMC Primary Care
1
BMC Public Health
1
BMJ
1
BMJ Open
1
Bontemps, S.
1
Borgeson, J. R.
1
Bourne, R.
1
Bousquet, P.
1
Bovet, P.
1
Bradshaw, C.
1
Brawerman, G.
1
Brawerman, R.
1
Breathe, part of the European Respiratory Society (ERS)
1
Brickley, E.
1
Brown, J.PR.
1
Brozek, J. L.
1
Buckley, P.
1
Bueno Fischer, G.
1
Bueno, P. et al.
1
Bundesministerium für Migration und Flüchtlinge
1
Bundeszentrale für gesundheitliche Aufklärung BzgA
1
Burnens, M.P.
1
Caixeta, R.
1
Calam, R.
1
Camargos, P. A.
1
Campbell, N.R.C.
1
Campell, H.
1
Canadian Cancer Society
1
Cancer
1
Caprara, G.
1
Cazzoletti, L.
1
Cedars-Sinai
1
Center for Disease Control and Prevention, World Health Organisation
1
Cesare, M.D.
1
CHADU
1
Chakaya, J.
1
Chan, K. Y.
1
Charvat, H. et al.
1
Chen, Y.
1
Cherney, K.
1
CHEST
1
Chiang, C. Y.
1
Chiolero, A.
1
Chou-Zen Giam
1
Christina Brandes-Barbier, Véronique Millot, Tomas Allen et al
1
Chung, K. F.
1
Circulation Research
1
Clark, A.M. et al.
1
Cleveland Clinic
1
Cloutier, M. M.
1
Cochrane Database of Systematic Reviews
1
Colette van Hees and Ben Naafs
1
Collins, T.E.
1
Connolly, M.A.
1
Cooper, P. J.
1
COPD: Journal of Chronic Obstructive Pulmonary Disease
1
Corella de Sousa, J.
1
Covill, N.
1
Cullinan, P.
1
Custovic, A.
1
D. A. Enarson, S. M. Kennedy, D. L. Miller, et al.
1
Daures, J.
1
Dave Woods and S. Mehtar
1
Dave, R.
1
Davies, J.S.
1
Davis, G.
1
Debas, Haile T.
1
Department of Health and Human Services
1
Department of Health: Republic of South Africa
1
Deschildre, A. et al.
1
Desula, O.O.
1
Dhurjati, R.
1
Diabete Care
1
Diabetes Qualified is the accredited training organisation of Diabetes Australia
1
Diabetes Research and Clinical Practice
1
diabetesafrica.org
1
Diego, I.
1
Directorate General of Health Services
1
Directorate General of Health Services Ministry of Health & Family Welfare Government of the People’s Republic of Bangladesh
1
Donald A Enarson, Susan M Kennedy, David L Miller
1
Donkor, Peter
1
DR
1
Dramowski, A.
1
Drugs for Neglected Diseases initiative DNDi
1
eClinicalMedicine
1
Egyakawa Ankomah, S.
1
Ehrlich, R.
1
El Ftouh, M.
1
El Gaafary, M.
1
El Hasnaoui, A., Rashid N., Lahlou A. et al.
1
El-Khani, A. et al.
1
Emirates Diabetes Endocrine Society - edes
1
EngenderHealth
1
ERJ Open Research, part of the European Respiratory Society (ERS)
1
Espira, L. M.
1
et.
1
Ethiopian Journal of Health Sciences
1
European Commission Humanitarian Aid
1
European Heart Journal
1
European Journal of allergy and clinical immunology: Volume59, Issue5 May 2004 Pages 469-478
1
European Multiple Sclerosis Platform
1
European Respiratory Journal, part of the European Respiratory Society (ERS)
1
European Respiratory Society
1
Everydayhealth Group
1
EXPERT REVIEW OF ANTICANCER THERAPY2020, VOL. 20, NO. 4, 271–278
1
Ezeudo, D.
1
F.Simona,E.Javellea ,A.Cabie, et al.
1
Fabian, D.
1
Faculty of Health Sciences
1
Fahim, H. I.
1
Farrukh, L.
1
Fay, K.A. et al.
1
Federici, M.
1
Feizi, H.
1
Fédération Internationale des Societés de la Croix-Rouge et du Croissant Rouge
1
Fielding, K.
1
Figueiredo, C. A.
1
Firth, J. et al.
1
Fitzgerald, D. A.
1
Fitzgerald, D.A. et al.
1
Flaxman, S.
1
Flor, L.S.
1
Flying Publisher
1
Forster, R.B.
1
Fowkes, G.F.
1
Frank, A.
1
Fritsche, A.
1
frontiers
1
Frontiers in Nutrition
1
Frontiers in Physiology
1
Fujiwara PI, Dlodlo RA, Ferroussier O, Nakanwagi-Mukwaya A, Cesari G, Boillot F.
1
Gambelunghe, A.
1
Garratt, A.
1
Gaveikaite, V.
1
Gawande, Atul
1
Gaziano, T. et al.
1
Gaziano, Thomas A.
1
Gelband, Hellen
1
Georgy, V.
1
German Agency for Quality in Medicine (ÄZQ)
1
German Diabetes Association (DDG)
1
German Doctors
1
German Gymnastics Federation (Deutscher Turner-Bund, DTB)
1
Ghosh, A.
1
Gil, A.
1
Glenn, B. E.
1
Global Allergy & Airways
1
Global Change Data Lab
1
Global Coalition for Circulatory Health
1
Global Health Media
1
Global Heart
1
Global Institute for Asthma
1
Global Polio Eradication Initiative GPEI
1
Godard, P.
1
Goh, N. S. L.
1
Gojka Roglic, Cherian Varghese, Leanne Riley et al.
1
Govender, K.
1
Goverment of the Netherlands
1
Government of India, Directorate General of Health Services, Public Health- International Health division
1
Government of Nigeria
1
Government of the Republic of Namibia
1
Gölz, S.
1
Greaves, C.J.
1
Green, R.
1
Grieger, L.
1
Grunstrom, C.
1
Guimaraes, Alice Soares
1
Gumbo, F.Z.
1
Guo, J.
1
Gupta, R.
1
Haahtela, T.
1
Haak, T.
1
Haileamlak, A.
1
Hall A.G.
1
Hambleton, I. R.
1
Hamers, R.
1
Han, K.
1
Hanas, R.
1
Hantera, M.
1
Harald T. Lutz Hassen A. Gharbi
1
Harding, J.L.
1
Harrison, V.
1
Harvey V. Fineberg
1
Hasan, K.
1
Hassanein M., Afandi B. et al.
1
Health and Environment Alliance
1
Health and Quality of Life Outcomes
1
Health Department: Republic of South Africa
1
Health Emergencies Programme
1
Heart Rhythm O2
1
HelpNow
1
Helthcare Improvement Scotland
1
Herdy, A.H.
1
Herman Woerdenbag
1
Hill, A.
1
Hjortdahl, Per.
1
Ho T., Cusack R.P., Chaudhary N. et al.
1
Hoines, K.
1
Hole, D.
1
Holmes, King K.
1
Holt, S.
1
Horton, Susan, et al.
1
Hosny, H.
1
Hou, D.
1
Hoy, R.
1
Hu, X.
1
Huffman, M. et al.
1
Human Rights Watch, International Harm Reduction Association, Canadian HIV
1
Human Rights Watch, International Harm Reduction Association, Canadian HIV/AIDS legal Network et al.
1
Hwang, J.
1
ICRC
1
IFRC
1
Iheanacho, I.
1
Indian Chest Society
1
Indian Journal of Ophthalmology 69(11):p 2932-2938, November 2021.
1
Infection Prevention and Control UHL, WHO Headquarters
1
Infectious Diseases Society of America
1
Institute for Clinical Effectiveness and Health Policy
1
Institute for Health Metrics and Evaluation - University of Washington
1
Institutional Repository for Information Sharing iris
1
International AIDS society
1
International Angiology
1
International Cancer Control Partnership
1
International Diabetes Federation (IDF)
1
International Journal of Chronic Obstructive Pulmonary Disease
1
International Journal of Tuberculosis and Lung Disease
1
International Pharmaceutical Federation (FIP)
1
International Primary Care Respiratory Group IPCRG
1
International Society of Nephrology
1
International Union Against Tuberculosis and Lung Disease (The Union)
1
Internet Interventions
1
Iris Onipede, Ellen Schmitt
1
Jackson, C. D.
1
Jamison, Dean T.
1
Jeebhay, M.F.
1
Jensen, C.
1
Jewell, C.P.
1
Jeyaseelan, S.M.
1
Jha, Prabhat
1
Jiang, N. et al.
1
Joe Schofield, Sarah Hess, Bandana Malhotra et al.
1
John Hopkins Medicine
1
John R. Perfect, William E. Dismukes, Francoise Dromer, et al.
1
John Wiley & Sons Australia, Ltd (Respirology)
1
Johns Hopkins Medicine
1
Jornal of Medical Internet Research JMIR Publication Published on 13.2.2023 in Vol 12 (2023)
1
Jose Bertolote, José Miguel Caldas de Almeida, Thomas Bornemann et al.
1
Jose Nkuni, Natasha Howard, Abraham Mnzava et al.
1
José Bertolote, Michelle Funk, Vladimir Poznyak et al.
1
Journal of Allergy and Clinical Immunology
1
Journal of Allergy and Clinical Immunology: Global
1
Journal of Cystic Fibrosis
1
journal of global health
1
Journal of the Royal Society of Medicine Open
1
Justin Cohen, Deepika Kandula, Bruno Moonen et al.
1
Kanukula, R. et al.
1
Karakiewicz, B.
1
Karmali, D.
1
Kengne, A.P. et al.
1
Kerdmongkol, P.
1
Khan, J.A.
1
Khawar Sana, M.
1
Kheder, A.B.
1
Kiley, J.
1
Kim, M.S.
1
King, D.
1
Kirenga, B.J.
1
Kistnasamy, B.
1
Kitchin, O.P. et al.
1
Knight, D.
1
Kobusingye, Olive
1
Kosinski, M.
1
Kotwas, A.
1
Kumah, E.
1
Kumar, R.
1
lagos acacia
1
Laisure, M.
1
Lakshmanan, S.
1
Lamond, E.
1
Lancet Commission
1
Lareau S.C., Fahy B. et al
1
Larson, M. C.
1
Larson, P. S.
1
Lee, J.H.
1
Leerapan, P.
1
Lenfant, C.
1
Lenney, W.
1
Leong, T. L.
1
Lesosky, M.
1
Leufkens, H.G.M. et al.
1
Levin, C.E. et al.
1
Li, J.T
1
Lin, J.
1
Lin, X.
1
Ling, S.
1
Lloyd, Linda
1
López-Jiménez, F.
1
M Mohsen Ibrahim, Albertino Damasceno
1
Maclean Soruco, Enrique y Eguivar, Mario A
1
Madkour, A.
1
Magitta, N.F.
1
Magwenzi, P.
1
Makanjuola, A. et al.
1
Management Science for Health MSH
1
Manne-Goehler, J. et al.
1
Mannino, D.M.
1
Margaret Grigg , Michelle Funk, Natalie Drew et al.
1
Marina Smelyanskaya, John Duncan
1
Markbreiter, J.
1
Marks, G. B.
1
Marx, N.
1
Masekala, R.
1
Masekela, R.
1
Masoli, M.
1
Mathioudakis, A.G.
1
Matsushita, K.
1
Mbanze, I.
1
Mbatchou Ngahane, B.H.
1
McCreanor, J.
1
McDonnell, J.
1
McKee, M.
1
McKeon, G.
1
Measles Initiative
1
MEDBOX Team
1
Media Production Archives
1
Medicines for Malaria Venture (MMV)
1
MedlinePlus
1
Mehra, R.
1
Melvyn Freeman, Michelle Funk, Soumitra Pathare et al.
1
MEPs Mobilising for Diabetes
1
Meya, D.B.
1
Médecins sans Frontières MSF
1
Middlehurst, A.
1
Miller, M. K.
1
Million Hearts
1
Minister of Health and Family Welfare Government of India
1
Ministry of Health & Family Welfare Government of India
1
Ministry of Health and Child Welfare
1
Ministry of Health and Child Welfare,Zimbabwe
1
Ministry of Health and Family Welfare (MoHFW) - India
1
Ministry of Health and Wellness
1
Ministry of Health Republic of Ghana
1
Ministry of Health Rwanda
1
Ministry of Health Singapore - Health Hub
1
Minja, N.W.
1
Minnesota Pollution Control Agency
1
Mishra, S.R.
1
Mock, Charles N.
1
Moen, A.
1
Mohammed A. , Putnis N. et al.
1
Mohan, V.
1
Molecular Diversity Preservation International MDPI
1
Momtazmanesh S., Chiou P.
1
Moraes Morelli, D.
1
Moreas Morelli, D.
1
Moreira Camargos, P. A.
1
Motshabi, P. et al.
1
Mörk, A-C.
1
MSF
1
MSF, Dubois, G.
1
Mugenyi, L.
1
Mugia, N.
1
Muhammad, S.A. et al.
1
Multidisciplinary Digital Publishing Institute (MDPI)
1
Murray, J.
1
Musaazi, J.
1
Mwanga, H.
1
MyHealth.Alberta.ca
1
Nagel, F.
1
Naidoo, N.
1
Naidoo, P.
1
Naik, N.
1
Naik, V.
1
Nakagaayi, D.
1
Nancy G Guerra, Ariel A Williamson, Beatriz Lucas-Molina
1
Nantanda, R.
1
Narula, J.
1
Nathan, R. A.
1
National Centre for Vector Borne Disease Control (NCVBDC)
1
National Department of Health, South Africa
1
National Health Mission
1
National Health Mission State Health Systems Resource Center- Kerala Academy of Pulmonary and Critical Care Medicine
1
National Institute for Health and Care Excellence
1
National Institute for Health and Care Excellence - NICE
1
National Institute for Occupational Safety and Health
1
National Istitute for Health Research
1
National Stroke Foundation
1
Naveed, A.
1
Ndarukwa, P.
1
Ndlovu, N.
1
Neaz, S.
1
Nejadghaderi, S.A.
1
Nelson, G.
1
Niedersächsisches Ministerium für Soziales, Gesundheit und Gleichstellung
1
Nieuwenhuijsen, M.J.
1
Nina Urwantzoff, Ellen Schmitt, Piet Reijer
1
Nugent, R.
1
Nugent, Rachel
1
Nunes da Cunha I., Autry E. et al
1
OECD
1
Official Journal of the Asian Pacific Society of Respirology
1
Ogle, G.
1
Ojji, D.B.
1
Olopade, C.O.
1
Oluwole, O.
1
Onyedum, C.C.
1
Open Heart
1
OpenWHO
1
Oregon State University - Linus Pauling Institute » Centro de Información de Micronutrientes
1
Oregon State University - Linus Pauling Institute » Micronutrient Information Center
1
Oregon State University - Linus Pauling Institute » 微量栄養素情報センター
1
Organisation de la Santé Mondiale OMS, Bureau Regional de l'Afrique
1
Organisation Mondiale de la Santé OMS
1
Organización Mundial de la Salud (OMS)
1
Organización Mundial de la Salud OMS
1
ORGANIZACIÓN MUNDIAL DE LA SALUD, ORGANIZACIÓN PANAMERICANA DE LA SALUD
1
Organização Mundial da Saúde (OMS)
1
Ostroff, J.L.
1
Ostroff, M.L.
1
Otchere, G.
1
Oxfam
1
Ozho, O.B.
1
Ozoh, O.
1
P.L.Perine, et al.
1
Paccaud, F. et al.
1
Pan American Health Organization PAHO, World Health Organization WHO
1
Pan, X.
1
Papadopoulos, E.
1
Papadopoulos, N.G.
1
Papana, A.
1
Parks, Will
1
Pearce, N.
1
Peiris, D.
1
Pennsylvania Department of Health
1
Pepper, M.
1
Peter Bakker
1
Pillay, S.
1
Pira E., Donato F., Maida L. et al.
1
Pitrez, P. M.
1
PLH
1
PLoS Medicine
1
PLOS Neglected Tropical Diseases
1
PLoS One
1
PLOS ONE, which is part of the Public Library of Science (PLOS)
1
Polatli, M.
1
Polidano, K., Wenning, B., Ruiz-Cadavid, A. et al.
1
Popov, T.
1
Prabhakaran, D.
1
Pradeepa, R.
1
Pressestelle der Beauftragten der Bundesregierung für Migration, Flüchtlinge und Integration
1
Primary Care Respiratory Journal
1
Ptaszek, L.M.
1
Public Health Reviews
1
rabhakaran, Dorairaj
1
Rajesh Upadhyay, Milind Y Nadkar, A Muruganathan
1
Ramnath, K.
1
Rangarajan, S. et al.
1
Rees, D.
1
Regional Office for Europe
1
Rehman, A.
1
Reid, G.
1
Reports and Data
1
Respiratory Medicine (2005) 99, 553–558
1
Respiratory Medicine (2006) 100, 616–621
1
Respiratory Research
1
Revista Latinoamericana de Desarrollo Económico
1
Richardson, C.R.
1
Risenga, S.M.
1
Robert Koch Institut RKI
1
Rodrigues, L.
1
Román-Rodríguez, M.
1
Rosengren, A.
1
Royal College of Physicians, London
1
Rubinstein, F.
1
Rudan, I.
1
Rumgay, H.
1
Rusakaniko, S.
1
Rwanda Biomedical Center
1
S. Bahendeka, S.Colagiuri, S. Mendis, et al.
1
Sagar, V.
1
Salehi, M.
1
Salim, H.
1
Salud Entre Culturas
1
Salvi S.
1
Salvi, S.
1
SAMJ
1
Santero, M.
1
Saratov Journal of Medical Scientific Research
1
Saudi Journal of Biological Sciences
1
Schatz, M.
1
Schokker, S.
1
Schütt, K. et al.
1
Schwalm, J.
1
Schwartz, L.
1
Sciences, A.
1
Scientific Animations Without Borders (SAWBO)
1
Scientific Cooperation Center "Interactive plus"
1
Scientific reports
1
Selroos, O.
1
Semmes, Oliver John
1
Sernikoff, S.
1
Sharif, Z.
1
Shield, K.
1
Shin, D.W. et al.
1
Shire
1
Siddharthan, T.
1
Silink, M.
1
Sin, D.D.
1
Singh, M.
1
Singh-Phulgenda, S., Dahal, P., Ngu, R. et al.
1
Slama, S.
1
SlideShare
1
Sliwa, K.
1
Smith, J.R.
1
Smokovski, I.
1
Smyth, A.
1
Social Sciences
1
Solidarités International
1
Soriano, J.B.
1
Soumitra Pathare, Michelle Funk, Melvyn Freeman et al.
1
Soumitra Pathare, Руби Холл, Michelle Funk et al.
1
South Africa Cystic Fibrosis Association (SACFA)
1
South African Cystic Fibrosis Association (SACFA)
1
South African Medical Journal (SAMJ)
1
Souto Medeiros, D. et al.
1
Springer
1
Springer Link
1
Springer Nature
1
Srisarakham, P.
1
Stefan Mauss, Thomas Berg, Jürgen Rockstroh et al.
1
Stelmach, R.
1
Stephens, J.W.
1
Stewart, C.
1
Stolbrink, M.
1
Stop TB Partnership. Working Group on TB
1
Sun, B-X.
1
Sur, P.J.
1
Susan M K Tan, Norazlin Kamal Nor, Loh Sit Fong, Suzaily Wahab
1
Svensson, K.
1
Szefler, S. J.
1
Tageldin, M.A.
1
Taright, S.
1
TB Care
1
Teach, S.J.
1
Temesgen, A. M.
1
Teresinha Mocelin, H.
1
Terzic, C.P. et al.
1
TEVA, Aktiv-mit-MS.de
1
The Alliance, unicef
1
The British Medical Journal (BMJ)
1
The Community Guide
1
The COPD Foundation
1
The COPD Foundation - South Africa
1
The Defeat-NCD Partnership
1
The Global Fund
1
The International Journal of Tuberculosis and Lung Disease
1
The Journal of Allergy and Clinical Immunology
1
The Journal of Allergy and Clinical Immunology: In Practice
1
The Lance Regional Health America
1
The Lancet Global Health Volume 11, Issue 2e218-e228February 2023
1
The Lancet Healthy Longevity Volume 2, Issue 6e340-e351June 2021
1
The Lancet Oncology
1
The Lancet Regional Health - Americas
1
The Lancet Respiratory Medicine
1
The New England Journal of Medecine
1
The Pan-African Society of Cardiology (PASCAR)
1
The Polio Global Eradication Initiative
1
The Royal Australian College of General Practitioners
1
The World Bank
1
Thembelihle Hlophe, S.
1
Thomas Jans Yesim Taneli Andreas Warnke
1
Thompson, J.L.
1
Tisiligianni, I.
1
Tonelli, M.
1
Trujillo, C.
1
Tsao, C.W.
1
Tsiligianni, I.
1
Tsilochristou, O.
1
Tufts University, Oxfam
1
Tze, P.
1
U. S. Centers for Disease Control and Prevention
1
U.S. Department of Health and Human Services
1
Ugurlu, M.
1
Ukwaja, K.N.
1
UN Children´s Fund
1
UN Children's Fund UNICEF
1
UN environment programme
1
UNDP
1
UNESCO
1
UNFPA
1
UNFPA, IFRC
1
Union Internationale Contre la Tuberculose et les Maladies Respiratoires
1
UNITAID Secretariat, World Health Organization
1
United Nations
1
United Nations Office for the Coordination of Humanitarian Affairs OCHA
1
United Nations Office on Drugs and Crime (UNODC)
1
United Nations Office on Drugs and Crime UNODC
1
United Nations UN
1
Uniting Combat Negleceted Tropical Diseases
1
University of Cape Town - South Africa
1
UNOPS, Stop TB Partnership
1
Urrutia-Pereira, M.
1
USAID
1
Valovirta, E.
1
van den Akker, M.
1
van den Born, B.
1
Van der Molen, T.
1
van Zandwijk, N.
1
Vasseur-Binachon, B.
1
Vats, S.
1
Venngange Inc.
1
Versus Arthritis
1
Vincent Gooskens
1
Volume 47, Issue Supplement_1 January 2024
1
Wadda, V.
1
Wali, S.
1
Walker, A.
1
Wallace, L.
1
Walters, S.
1
Wan, C.
1
Wander, P.L.
1
Wang, H.
1
Wang, H.H.X.
1
Wang, X-R.
1
Wang, y.
1
Watt, G.
1
Webb, D.
1
Weiberg, E.
1
Weinberg, E.G.
1
Wenzel, S. E.
1
Whelton, P.K. et al.
1
WHO Regional Office for Europe
1
WHO Regional Office for Europe United Nations City
1
WHO Regional Office for South-East Asia
1
WHO Regional Office for the Eastern Mediterranean
1
WHO, UNICEF, UNODC, et al.
1
Wiliams, S.
1
Willemse, B.
1
Winter, S.
1
WiRED International
1
Wolrd Health Organisation (WHO)
1
Wong, M.L. et al.
1
World Allergy Organization Jornal Volume 13, Issue 6100130June 2020
1
World Allergy Organization-IAACI (WAO)
1
World Bank Group
1
World Health Organization (WHO), Regional Office for South-East Asia
1
World Health Organisation
1
World Health Organisation WHO
1
World Health Organisation Zimbabwe
1
World Health Organisation, International Labour Organization
1
World Health Organization ( WHO), Regional Office for South-East-Asia
1
World Health Organization (WHO) Regional Office for Europe
1
World Health Organization (WHO), International Telecommunication Union (ITU)
1
World Health Organization (WHO)
1
World Health Organization - Regional Office for South-East Asia
1
World Health Organization - Regional Office for South-East Asia
1
World Health Organization Africa WHO
1
World Health Organization South- East Asia Journal of Public Health
1
World Health Organization WHO African Region
1
World Health Organization WHO, Regional Office for Africa
1
World Health Organization WHO, Regional Office for Europe
1
World Health Organization WHO, Regional Office of Africa
1
World Health Organization, Pan American Health Organization
1
World Health Organization, Regional Office for South-East Asia
1
World Health Organization, Regional Office for the Americas
1
World Health Organization, Regional Office South-East Asia
1
World Health Organization, UNAIDS, United Nations Office on Drugs and Crime
1
World Health Organization, World Heart Federation, World Stroke Organization
1
World Health Organization/Europe
1
World Organisation for Animal Health, World Health Organization (WHO), Food and Agriculture Organization (FAO)
1
Worldwide Hospice Palliative Care Alliance
1
Xiaoyan Ke, Jing Liu
1
Xu,Y.
1
Yaria, J.
1
Yassi, A.
1
Ye, X.
1
Yimer, G. et al.
1
Yon, D.K. et al.
1
Yoo, J.E.
1
Yoshimoto, C.
1
Yu, J. et al.
1
Yusuf, S.
1
Yuyun, M.F.
1
Yvonne Bonomo, Cornelius Goos, John Howard et al.
1
Zabielska, P.
1
Zanolin, M.E.
1
Zar, H.J.
1
Zayeri, F.
1
Zhang, H-X.
1
Zhang, S.
1
Zhang, X.
1
Zhang, Y.
1
Zhu, Y. et al.
1
«Центр анализа политики здравоохранения», World Health Organization, Schweizerische Eidgenossenschaft
1
Агентство США по международному развитию бюро всемирного здравоохранения отдел здоровья, инфекционных заболеваний и питания.
1
Александрович Ю.С., Алексеева Е.И., Бакрадзе М.Д., et al.
1
Альянс громадського здоров'я, Drop in center
1
Альянс громадського здоров'я, Drop in center
1
Анатолий Волик
1
Бара Бука
1
Бачило Е. В., Барыльник Ю. Б.
1
Бачило Е. В., Барыльник Ю. Б., Антонова А. А.
1
Благиных Е. С.
1
В.Ф. Беженарь, Э.К. Айламазян, И.Е. Зазерская et al.
1
Васильева Лидия Львовна
1
Всемирная организация здравоохранения (Европейское)
1
ГБОУ ВПО «Нижегородская государственная медицинская академия»
1
ГБОУ ВПО ЮУГМУ Министерство Здравоохранения России Кафедра психиатрии факультета дополнительного образования
1
Гос. науч. центр соц. и судебной психиатрии.
1
ГУЗ «Центр медицинской профилактики департамента здравоохранения Краснодарского края»
1
Департамент по ВИЧ/СПИД, Департамент «Остановить ТБ», Всемирная организация здравоохранения
1
Детский Фонд ООН, unicef, Columbia University MAILMAN SCHOOL OF PUBLIC HEALTH
1
Е.В. Макушкин, Н.К. Демчева, Н.А. Творогова
1
Е.В. Малинина, И.В. Забозлаева, Т.Н. Саблина et al.
1
Е.Г. Карташова
1
европейская федерация головной боли, всемирная организация здравоохранения, всемирный альянс головной боли et a.
1
Европейский центр мониторинга наркотиков и наркозависимости, Publications Office of the European Union
1
Ж.В. Альбицкая
1
Жукова О. А., Кром И. Л., Барыльник Ю. Б.
1
Зайратъянц О.В., Каниболоцкий А.А., Михалева Л.М, et al.
1
Зайратьянц О.В., Cамсонова М.В., Михалева Л.М., et al.
1
Законодательная Дума Томской области
1
И.А. Карпов1, А.С. Иванов2, И.В. Юркевич et al.
1
Камкин Евгений Геннадьевич, Костенко Наталья Алексеевна et. al.
1
Карелина Д. Д., Кром И. Л., Барыльник Ю. Б.
1
Кекелидзе З.И., Пасынкова Ю. Г., Бедина И.А.
1
Лукина Е. В., Чернышева О. А., Елисеева В. А.
1
Лукина Е.В. ,Кузнецова Д.Е.
1
Между- народный Альянс по ВИЧ/СПИД в Украине, фонд «Общественное здоровье»
1
Международный Союз по борьбе с туберкулезом и заболеваниями легких
1
Межрегиональная ассоциация по клинической микробиологии и антимикробной химиотерапии (МАКМАХ)
1
Министерство здравоохранения Российской Федерации
1
Науч. центр психического здоровья РАМН
1
Науч. центр психического здоровья РАМН.
1
Раздорская В. В., Воскресенская О. Н., Юдина Г. К.
1
Разработано и издано Открытым Институтом Здоровья (ОИЗ) в рамках проекта глобус
1
С. Н. Авдеев , Е. В. Волчкова , О. М. Драпкина, et al.
1
Самойлова Д. Д., Барыльник Ю. Б.
1
Союз охраны психического здоровья
1
Стопкоронавирус.рф — Официальный интернет-ресурс для информирования населения по вопросам коронавируса (COVID-19)
1
Т.Дж. Стайнер, К. Пемелера, Р. Йенсен et al.
1
Тургунбаев Д.Д., Артыкбаев А.Ш., Кадырова Н.
1
ФГБУ «Государственный научный центр социальной и судебной психиатрии им. В.П. Сербского» Минздрава России
1
Федеральное государственное бюджетное научное учреждение научный центр психического здоровья
1
Штат Нью-Йорк Отдел охраны психического здоровья
1
Эко-Вектор
1
Эмма Роган, Элизабет Кэсилингем, Клод Бербек
1
ЮНЭЙДС
1
Ястребов В.С., Гонжал О.А., Тюменкова Г.В et al.
1
Publication Years
1980-1989
2
1990-1999
9
2000-2009
92
2010-2019
380
2020-2025
656
Category
Public Health
753
Clinical Guidelines
266
Countries
115
Capacity Building
29
Women & Child Health
27
Key Resources
26
Pharmacy & Technologies
10
Toolboxes
NCDs
562
COVID-19
104
Mental Health
77
Rapid Response
38
NTDs
26
2.0 Rapid Response
23
TB
18
Refugee
17
Caregiver
13
Malaria
10
HIV
9
Conflict
9
Polio
9
Ebola & Marburg
8
Planetary Health
7
Global Health Education
7
Cholera
6
Natural Hazards
5
Pharmacy
5
Zika
4
Disability
3
AMR
2
Specific Hazards
1

Many low-resource settings have a shortage of physicians and health workers. (1) In order to provide patient-centred continuous care more effectively, primary care systems can include team-based care strategies in their clinic workflows and protocols. Team-based care uses multidisciplinary teams (wh...ich may involve new staff, or the shifting of tasks among existing staff). Teams can include patients themselves, primary care physicians, and other allied health professionals, such as nurses, pharmacists, counsellors, social workers, nutritionists, community health workers, or others. Teams reduce the burden on physicians by utilizing the skills of trained health workers. Strong evidence shows that team-based care is effective in improving hypertension control among patients in a cost-effective way. (2) Some amount of task shifting/team-based care is already taking place in many settings; this module provides further guidance on how to maximize this approach for greater impact.
more


Global Hear, March 2014, Vol. 9 no.1

Weekly epidemiological record/ Relevé épidémiologique hebdomadaire 4 AUGUST 2017, 92th YEAR / 4 AOÛT 2017, 417-436

The report aims to help policy-makers and programme managers identify the areas that need attention and to work towards effective implementation and enforcement of policies and legislations. The need for alcohol policy-specific infrastructures to support the alcohol policy process, including designa...ted responsible agency, policy and strategy, and law and regulation, is also required at the country level.
The report is presented in three sections. Section 1 gives an insight to the alcohol consumption situation in the WHO South-East Asia Region and cites the alcohol-related problems that the Region is facing. Section 2 illustrates the policy situation in the 10 areas of national action identified in the Global Strategy to Reduce the Harmful Use of Alcohol and gives specific recommendations pertaining to these areas. Section 3 provides overall recommendations. more
The report is presented in three sections. Section 1 gives an insight to the alcohol consumption situation in the WHO South-East Asia Region and cites the alcohol-related problems that the Region is facing. Section 2 illustrates the policy situation in the 10 areas of national action identified in the Global Strategy to Reduce the Harmful Use of Alcohol and gives specific recommendations pertaining to these areas. Section 3 provides overall recommendations. more
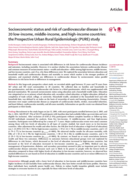
Socioeconomic status is associated with differences in risk factors for cardiovascular disease incidence and outcomes, including mortality. However, it is unclear whether the associations between cardiovascular disease and common measures of socioeconomic status—wealth and education—differ among... high-income, middle-income, and low-income countries, and, if so, why these differences exist. We explored the association between education and household wealth and cardiovascular disease and mortality to assess which marker is the stronger predictor of outcomes, and examined whether any differences in cardiovascular disease by socioeconomic status parallel differences in risk factor levels or differences in management.
more
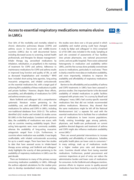
Over 90% of the morbidity and mortality related to chronic obstructive pulmonary disease (COPD) and asthma occurs in low-income and middle-income countries (LMICs) due to well documented factors including decreased access to screening, trained health professionals, and therapies for disease manageme...nt. Inhaler therapy (eg, aerosolised medications by inhalation, nebulisation, or propellant) is the mainstay of treatment for COPD and asthma. Adherence to maintenance medications for COPD and asthma results in improved lung function and quality of life, as well as decreased hospitalisation and mortality. WHO have included short-acting beta-agonists, long-acting muscarinic antagonists, and inhaled corticosteroids on the essential medications list, with a target goal of achieving 80% availability of these medications in public and private facilities. However, despite these efforts, accessibility, and affordability of medications for COPD and asthma remains scarce.
more

Background
Cardiovascular diseases (CVDs) are one of the global leading causes of concern due to the rising prevalence and consequence of mortality and disability with a heavy economic burden. The objective of the current study was to analyze the trend in CVD incidence, mortality, and mortality-to-...incidence ratio (MIR) across the world over 28 years.
Methods
The age-standardized CVD mortality and incidence rates were retrieved from the Global Burden of Disease (GBD) Study 2017 for both genders and different world super regions with available data every year during the period 1990–2017. Additionally, the Human Development Index was sourced from the United Nations Development Programme (UNDP) database for all countries at the same time interval. The marginal modeling approach was implemented to evaluate the mean trend of CVD incidence, mortality, and MIR for 195 countries and separately for developing and developed countries and also clarify the relationship between the indices and Human Development Index (HDI) from 1990 to 2017.
Results
The obtained estimates identified that the global mean trend of CVD incidence had an ascending trend until 1996 followed by a descending trend after this year. Nearly all of the countries experienced a significant declining mortality trend from 1990 to 2017. Likewise, the global mean MIR rate had a significant trivial decrement trend with a gentle slope of 0.004 over the time interval. As such, the reduction in incidence and mortality rates for developed countries was significantly faster than developing counterparts in the period 1990–2017 (p < 0.05). Nevertheless, the developing nations had a more rather shallow decrease in MIR compared to developed ones.
Conclusions
Generally, the findings of this study revealed that there was an overall downward trend in CVD incidence and mortality rates, while the survival rate of CVD patients was rather stable. These results send a satisfactory message that global effort for controlling the CVD burden was quite successful. Nonetheless, there is an urgent need for more efforts to improve the survival rate of patients and lower the burden of this disease in some areas with an increasing trend of either incidence or mortality.
more

Air pollution is the top environmental threat to health in Europe. It leads to hundreds of thousands premature deaths per year and billions of Euros in health costs.

Diabetes Online courses - Global Health Media

Non-communicable diseases (NCDs) are major global public health concerns that cause nearly three-quarters of the burden of mortality worldwide. Cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes alone account for over eight out of ten NCD deaths. To alleviate this huge burde...n, the Sustainable Development Goals (SDG) aimed to reduce premature mortality from non-communicable diseases by one-third.
more

This report includes analysis from informal regional consultations in the African Region, the Caribbean and North America, Latin America, South-East Asia Region, European Region, Eastern Mediterranean Region, alongside three forums in the Western Pacific Region. It analyses the overarching similarit...ies, regional nuances and priorities raised across the six WHO regions for the meaningful engagement of individuals with lived experience.
It is the second publication in the WHO Intention to action series, which aims to enhance the limited evidence base on the impact of meaningful engagement and address the lack of standardized approaches on how to operationalise meaningful engagement. The Intention to action series aims to do this by providing a platform from which individuals with lived experience, and organizational and institutional champions, can share solutions, challenges and promising practices related to this cross-cutting agenda. The Intention to action series also aims to provide powerful narratives, inspiration and evidence towards the Fourth United Nations High Level Meeting on NCDs in 2025 and achieving the 2030 United Nations Sustainable Development Goals (SDGs).
more
The Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013-2020 by the World Health Organization (WHO) outlines a comprehensive strategy to address the global rise in noncommunicable diseases (NCDs), including cardiovascular diseases, cancer, chronic respiratory diseases,... and diabetes.
more
Noncommunicable diseases (NCDs) – chief among them, cardiovascular diseases (heart disease and stroke), cancer, diabetes and chronic respiratory diseases – along with mental health, cause nearly three quarters of deaths in the world. Their drivers are social, environmental, commercial and geneti...c, and their presence is global. Every year 17 million people under the age of 70 die of NCDs, and 86% of them live in low- and middle-income countries (LMICs).
more
The World Health Organization's fact sheet on noncommunicable diseases (NCDs) highlights that NCDs, such as cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes, are responsible for 74% of all global deaths, totaling 41 million annually. Notably, 86% of premature NCD deaths (...before age 70) occur in low- and middle-income countries. Key risk factors include tobacco use, physical inactivity, harmful alcohol consumption, unhealthy diets, and air pollution. The WHO emphasizes the importance of preventive measures, early detection, and comprehensive healthcare strategies to address the growing NCD burden.
more
An integrated approach is particularly important for low-resource settings for efficient use of limited resources. The course contents will include risk factors, clinical course, guidance and protocols for diagnosis, management and referral as needed for NCDs in PHC. SEARO NCD PEN-HEARTS is a series... of four courses with the other three courses focusing on Hearts of NCD: an integrated approach to management of NCDs in PHC, diabetic foot care and palliative care that will enable the learner to plan and deliver NCD services.
more

The document outlines the 2019 update to the South African guideline for managing chronic obstructive pulmonary disease (COPD). It emphasizes the importance of early diagnosis, prevention through smoking cessation, use of bronchodilators as primary pharmacotherapy, and a comprehensive approach to pa...tient care including pulmonary rehabilitation and the management of comorbidities. The guideline also covers recommendations for handling acute exacerbations, surgical interventions, and long-term treatment options.
more
The state of diabetes treatment coverage in 55 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 680 102 adults 2021
Flood, D.; Seiglie, J.A.; Dunn, M.; et al.
The Lancet Healthy Longevity Volume 2, Issue 6e340-e351June 2021
(2021)
CC2
Approximately 80% of the 463 million adults worldwide with diabetes live in low-income and middle-income countries (LMICs). A major obstacle to designing evidence-based policies to improve diabetes outcomes in LMICs is the scarce availability of nationally representative data on the current patterns... of treatment coverage. The objectives of this study were to estimate the proportion of adults with diabetes in LMICs who receive coverage of recommended pharmacological and non-pharmacological diabetes treatment; and to describe country-level and individual-level characteristics that are associated with treatment.
more


The Committee examined the clinical development of Ebola virus vaccines and conducted an inventory of available data on their safety. It also reviewed 3 generic issues: updating a global strategy on vaccine safety, use of a network of distributed data ... to monitor the safety of vaccines and case studies of communication about the safety of human papillomavirus (HPV) vaccines.
Weekly epidemiological record/Relevé épidémiologique hebdomadaire 12 JULY 2019, 94th YEAR / 12 JUILLET 2019, 94e ANNÉENo 28, 2019, 94, 309–316
more
A Project by
medbox @ 2025