Filter
2174
Text search:
funding
update
Featured
217
631
Language
Document type
1017
485
267
162
124
50
41
19
5
2
Countries
134
59
54
53
51
48
46
44
41
40
40
39
36
36
31
30
29
29
26
26
26
24
23
22
22
21
21
18
18
17
17
15
15
14
13
12
12
12
11
10
10
10
9
9
9
8
8
7
7
6
6
6
6
6
6
5
5
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
838
155
149
114
113
23
17
1
Toolboxes
181
129
101
94
91
85
68
54
53
51
50
50
48
48
44
42
40
34
32
31
21
20
20
4
2
1
1

This Communication Guide for Malaria Control Interventions is aligned with Tanzania’s Malaria Strategic Plan (2015–2020) and provides comprehensive guidance on the implementation of Social and Behaviour Change Communication (SBCC) for the prevention, diagnosis and treatment of malaria. It is int
...

This UNHCR guidance note provides comprehensive recommendations for the prevention and control of malaria in refugee settings worldwide. Aligned with the WHO Global Technical Strategy for Malaria, it outlines strategies to ensure access to effective prevention, diagnosis and treatment, implement sus
...

This Malaria Surveillance Assessment Toolkit implementation reference guide is a comprehensive reference document, as well as a step by-step guide. It aligns and adapts available tools into a single set of standardized tools, which can be used to conduct malaria surveillance assessments across all t
...

Clinical Pharmacology: Advances and Applications, 2025:17 29–47

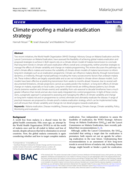
Malaria Journal (2021) 20:190

Reprogramming examples for GC7. This document supports the introduction of climate change-related interventions
into programs to reduce transmission of malaria and protect vulnerable populations.

The National Strategic Plan for Malaria Elimination 2021–2025 outlines Bangladesh’s roadmap to achieve zero indigenous malaria cases by 2030, with an interim goal to reduce transmission to near-zero levels by 2025. The strategy builds upon earlier successes in malaria control and shifts focus to
...

The framework recommends expanded coverage of malaria diagnostic and treatment services, intensified vector control to drive down transmission, strengthened malaria surveillance, and increased transborder collaboration, especially in terms of efforts to control the sale and use of artemisinin monoth
...

Offering additional pre-exposure prophylaxis (PrEP) choices has the potential to increase uptake and effective use of PrEP, and of HIV prevention overall, as it allows people to choose a method that they prefer.
In this guideline, WHO recommends an offering long-acting injectable lenacapavir (LEN
...

Guidelines on lenacapavir for HIV prevention and testing strategies for long-acting injectable pre-exposure prophylaxis. Web Annex B

The Ghana National Malaria Strategic Plan 2021–2025 aims to reduce malaria mortality by 90% and malaria cases by 50% (using 2019 as baseline) and to achieve pre-elimination in at least six districts by 2025. The plan focuses on scaling up prevention measures like distributing insecticide-treated n
...
The National Malaria Elimination Strategic Plan (NMESP) 2024–2028 of Ghana outlines the country’s roadmap to shift from malaria control to elimination. Despite major progress—like reducing malaria deaths from nearly 2,800 in 2012 to 151 in 2022—malaria remains a major public health challenge
...
The National Strategic Plan on Malaria Prevention and Elimination Period 2021 – 2025 seeks to build on the previous national successes of the National Institute of Malariology, Parasitology, and Entomology (NIMPE) while addressing current challenges to reduce the overall burden of malaria in the S
...
The Rwanda Malaria Strategic Plan 2020–2024 outlines Rwanda’s national strategy to reduce malaria morbidity and mortality by at least 50% compared to 2019 levels. The vision is a malaria-free Rwanda contributing to socioeconomic development.
The plan includes strengthening prevention through lo
...

This toolkit suggests several approaches to addressing technology
access disparities. At its core is a comprehensive checklist that helps
teams systematically evaluate their current practices and identify
opportunities for improvement. This structured self-assessment
tool spans both team-level a
...

This toolkit is a comprehensive set of practical tools and resources designed to support country-level risk communication and community engagement (RCCE) practitioners, decision-makers and partners to plan and implement readiness and response activities for Ebola disease outbreaks. The toolkit conta
...

This toolkit is a comprehensive set of practical tools and resources designed to support country-level risk communication and community engagement (RCCE) practitioners, decision-makers, and partners to plan and implement readiness and response activities for yellow fever outbreaks. The toolkit conta
...

This toolkit is a comprehensive set of practical tools and resources designed to support country-level risk communication and community engagement (RCCE) practitioners, decision-makers, and partners to plan and implement readiness and response activities for yellow fever outbreaks. The toolkit conta
...

This guide provides strategic direction for host countries, event organizers, health authorities, and key stakeholders to effectively plan and conduct Simulation Exercises (SimEx) and After Action Reviews (AARs) for mass gathering events. Packed with practical tools, it empowers users to seamlessly
...