Filter
8607
Filtered Results: 8607
Text search:
Project
Management
Featured
Recommendations
774
New Publications
2352
Language
Document type
No document type
4824
Studies & Reports
1445
Guidelines
1052
Manuals
489
Strategic & Response Plan
361
Training Material
166
Fact sheets
144
Situation Updates
72
Infographics
15
Brochures
14
Resource Platforms
14
Online Courses
8
Videos
2
App
1
Countries / Regions
Global
369
India
318
Kenya
254
Sierra Leone
189
Nepal
176
Myanmar / Burma
176
Nigeria
173
Uganda
172
Liberia
171
Ethiopia
167
Western and Central Europe
158
South Africa
150
Malawi
134
Bangladesh
131
Zambia
131
Tanzania
119
Rwanda
117
Africa
117
Syria
110
Ghana
103
Congo, Democratic Republic of
102
Namibia
90
Latin America and the Carribbean
86
Indonesia
86
Ukraine
81
Philippines
72
Haiti
67
South Sudan
65
Guinea
62
Senegal
61
Eastern Europe
60
Mozambique
54
South–East Asia Region
54
Lesotho
52
Asia
50
Cambodia
49
Burkina Faso
48
Zimbabwe
45
Germany
44
Cameroon
39
Yemen
38
West and Central Africa
35
Benin
34
East and Southern Africa
34
Botswana
34
Russia
33
Venezuela
30
Pakistan
27
Middle East and North Africa
26
Eastern Europe and Central Asia
26
Lebanon
25
Afghanistan
24
Brazil
24
Central African Republic
24
Jordan
21
Madagascar
21
Eswatini/ Swaziland
21
Colombia
20
Thailand
19
Mali
19
Somalia
18
Côte d’Ivoire / Ivory Coast
17
China
16
Sudan
16
Tajikistan
15
USA
15
Western Pacific Region
15
Vietnam
15
Iraq
14
Laos
13
Moldova
12
Albania
10
Peru
10
Chad
10
Turkey
9
Burundi
9
Sri Lanka
9
Chile
8
Iran
8
Niger
8
Papua New Guinea
8
Palestine
8
Georgia
8
Angola
8
North Macedonia
7
Togo
7
Armenia
7
Timor Leste/ East Timor
6
Gambia
6
Kyrgyzstan
6
Southern Africa
6
Argentina
6
Libya
6
Mexico
5
El Salvador
5
Paraguay
5
Bolivia
5
Kazakhstan
4
Jamaica
4
Spain
4
Romania
4
Honduras
4
Bhutan
4
Ecuador
4
Switzerland
3
Serbia
3
Estonia
3
Croatia
3
North America
3
Turkmenistan
3
Japan
3
France
3
Mauritius
3
Belarus
3
Greece
3
Poland
3
North Korea
2
Canada
2
Fiji
2
Congo-Brazzaville
2
Uzbekistan
2
Morocco
2
Dominican Republic
2
Guinea-Bissau
2
Hungary
2
Lithuania
2
Saudi Arabia
2
Gabon
2
Belgium
2
United Kingdom
2
Portugal
2
Nicaragua
2
Egypt
2
Guatemala
2
Singapore
1
Malaysia
1
Vanuatu
1
Mongolia
1
Qatar
1
Bulgaria
1
Mauritania
1
Italy
1
Uruguay
1
Denmark
1
Tunisia
1
Azerbaijan
1
Bosnia and Herzegovina
1
Belize
1
Costa Rica
1
Guyana
1
Panama
1
Djibouti
1
Solomon Islands
1
Authors & Publishers
Publication Years
Category
Countries
3238
Key Resources
641
Clinical Guidelines
528
Women & Child Health
455
Public Health
451
Capacity Building
186
Pharmacy & Technologies
84
Annual Report MEDBOX
3
Toolboxes
COVID-19
625
Mental Health
579
HIV
562
TB
402
Disability
390
Planetary Health
389
Ebola & Marburg
281
Conflict
276
Caregiver
259
AMR
226
NTDs
215
Global Health Education
164
Refugee
163
Rapid Response
162
Pharmacy
146
Natural Hazards
145
NCDs
135
Health Financing Toolbox
108
Malaria
101
2.0 Rapid Response
97
Specific Hazards
66
Cholera
54
Zika
46
Social Ethics
40
Polio
40
Typhoon
7
South Sudan
2

Africa’s health sector is facing an unprecedented financing crisis, driven by a sharp decline of 70% in Official Development Assistance (ODA) from 2021 to 2025 and deep-rooted structural vulnerabilities. This collapse is placing immense pressure on Africa’s already fragile health systems as ODA ...

Small drinking-water supplies commonly experience operational, managerial, technical and resourcing challenges that impact their ability to deliver safe and reliable services. The needs and opportunities associated with these supplies therefore warrant explicit consideration in policies and regulati...
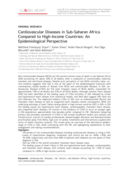
Non-communicable diseases (NCDs) are the second common cause of death in sub-Saharan Africa (SSA) accounting for about 35% of all deaths, after a composite of communicable, maternal, neonatal, and nutritional diseases. Despite prior perception of low NCDs mortality rates, current evidence suggests t...

Primary health care offers a cost–effective route to achieving universal health coverage (UHC). However, primary health-care systems are weak in many low- and middle-income countries and often fail to provide comprehensive, people-centred, integrated care. We analysed the primar...




Examples of small-scale disinfection products for safe drinking water
Handbook of HUMANITARIAN HEALTH CARE LOGISTICS Designing the Supply Network and Managing the Flows of Information and Health Care Goods in Humanitarian Assistance during Complex Political Emergencies

Provisional recommendations May 2014

Sector Environmental Guidelines, Full technical Update


SODIS manual - updated version
The SODIS manual contains detailed information about technical and promotional aspects of the SODIS method.
Former version also available in French, Portuguese, Spanish, Uzbek, Russian


Considerations for implementing and adjusting public health and social measures in the context of COVID-19
recommended
interim guidance, 14 June 2021
This document is intended for national authorities and decision makers in countries that have introduced large scale public health and social measures. It offers guidance for adjusting public health and social measures, while managing the risk of a resurgence of cases...



