Filter
2451
Filtered Results: 2451
Text search:
antiretroviral
treatment
guidelines
Featured
Recommendations
226
New Publications
712
Language
Document type
No document type
1681
Guidelines
303
Studies & Reports
257
Manuals
77
Strategic & Response Plan
49
Training Material
37
Fact sheets
25
Situation Updates
10
Infographics
7
Resource Platforms
2
Brochures
1
App
1
Online Courses
1
Countries / Regions
India
105
Kenya
97
South Africa
87
Tanzania
71
Zambia
70
Malawi
59
Ethiopia
59
Nigeria
53
Uganda
53
Namibia
52
Global
46
Nepal
45
Rwanda
41
Africa
40
Liberia
35
Western and Central Europe
34
Lesotho
33
Ukraine
32
Myanmar / Burma
32
Ghana
29
Zimbabwe
28
Sierra Leone
27
Latin America and the Carribbean
26
Eastern Europe
25
Asia
21
Cambodia
19
Botswana
18
Bangladesh
17
Russia
17
Mozambique
16
Philippines
14
Burkina Faso
12
Indonesia
12
Senegal
11
Eswatini/ Swaziland
11
South–East Asia Region
10
Argentina
9
Benin
8
Cameroon
8
Congo, Democratic Republic of
8
Paraguay
8
East and Southern Africa
8
Albania
7
Brazil
7
Georgia
7
Colombia
6
Pakistan
6
Thailand
5
Syria
5
Haiti
5
Venezuela
5
Germany
5
Southern Africa
5
Vietnam
5
Tajikistan
4
West and Central Africa
4
Bolivia
4
Sudan
4
South Sudan
4
North Macedonia
3
Peru
3
Guinea
3
Armenia
3
Somalia
3
El Salvador
2
Laos
2
Estonia
2
Afghanistan
2
Middle East and North Africa
2
Western Pacific Region
2
Eastern Europe and Central Asia
2
Moldova
2
Yemen
2
Romania
2
Central African Republic
2
Angola
2
Libya
2
Ecuador
2
Switzerland
1
Timor Leste/ East Timor
1
Gambia
1
Chile
1
Iran
1
Canada
1
Niger
1
Burundi
1
Qatar
1
Bulgaria
1
USA
1
Guinea-Bissau
1
Jordan
1
Saudi Arabia
1
North America
1
Turkmenistan
1
Jamaica
1
Belgium
1
Belarus
1
Côte d’Ivoire / Ivory Coast
1
Lebanon
1
Sri Lanka
1
Djibouti
1
Egypt
1
Palestine
1
Mali
1
Bhutan
1
Iraq
1
Authors & Publishers
Publication Years
Category
Countries
1050
Clinical Guidelines
232
Women & Child Health
127
Public Health
73
Capacity Building
59
Key Resources
52
Pharmacy & Technologies
24
Annual Report MEDBOX
1
Toolboxes
HIV
702
TB
326
Caregiver
53
Pharmacy
50
Mental Health
43
COVID-19
41
AMR
31
Refugee
27
Conflict
27
NTDs
24
NCDs
19
Ebola & Marburg
17
Disability
13
Global Health Education
12
Health Financing Toolbox
11
Polio
10
Rapid Response
9
Natural Hazards
6
Malaria
6
Social Ethics
5
Planetary Health
4
2.0 Rapid Response
2
Zika
2

In 2015, the United Nations set important targets to reduce premature
cardiovascular disease (CVD) deaths by 33% by 2030. Africa disproportionately
bears the brunt of CVD burden and has one of the highest risks of dying
from non-communicable diseases (NCDs) worldwide. There is currently
an epide...
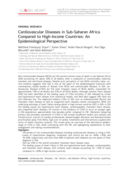
Non-communicable diseases (NCDs) are the second common cause of death in sub-Saharan Africa (SSA) accounting for about 35% of all deaths, after a composite of communicable, maternal, neonatal, and nutritional diseases. Despite prior perception of low NCDs mortality rates, current evidence suggests t...

AIDS Behav. 2022 Feb;26(2):375-384.doi: 10.1007/s10461-021-03391.
A community health worker (CHW) model can promote HIV prevention and treatment behaviors,
especially in highly mobile populations. In a fishing community in Rakai, Uganda, the Rakai
Health Sciences Program implemented a communit...









National Strategic Plan for HIV 2015-2020 Malawi
recommended




Over 2 million children worldwide are living with HIV infection and 95% reside in sub-Saharan Africa with the majority infected through mother-to-child transmission. Infected children have a high mortality with 50% dying by 2 years of age. Their clinical presentation includes common childhood infect...



This document provides an overview of key considerations for the provision of the HIV continuum of care in the context of displaced people from Ukraine in the EU/EEA. This document has two aims: firstly, to outline what is known of the Ukrainian HIV epidemic, and secondly, to use the HIV continuum o...