
Climate Solutions Double as Health Interventions

 , ,
, ,
Abstract
:1. Introduction
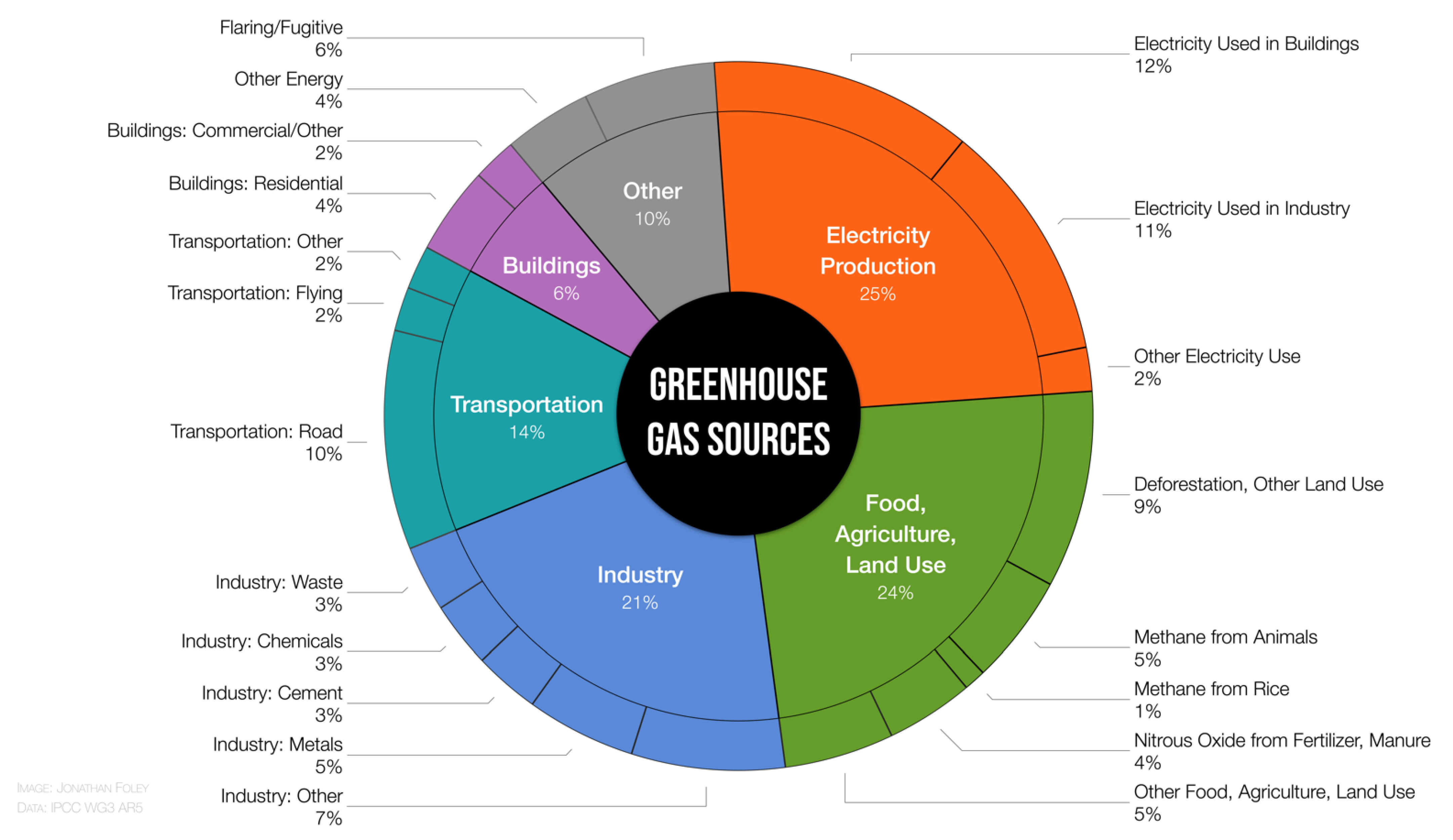
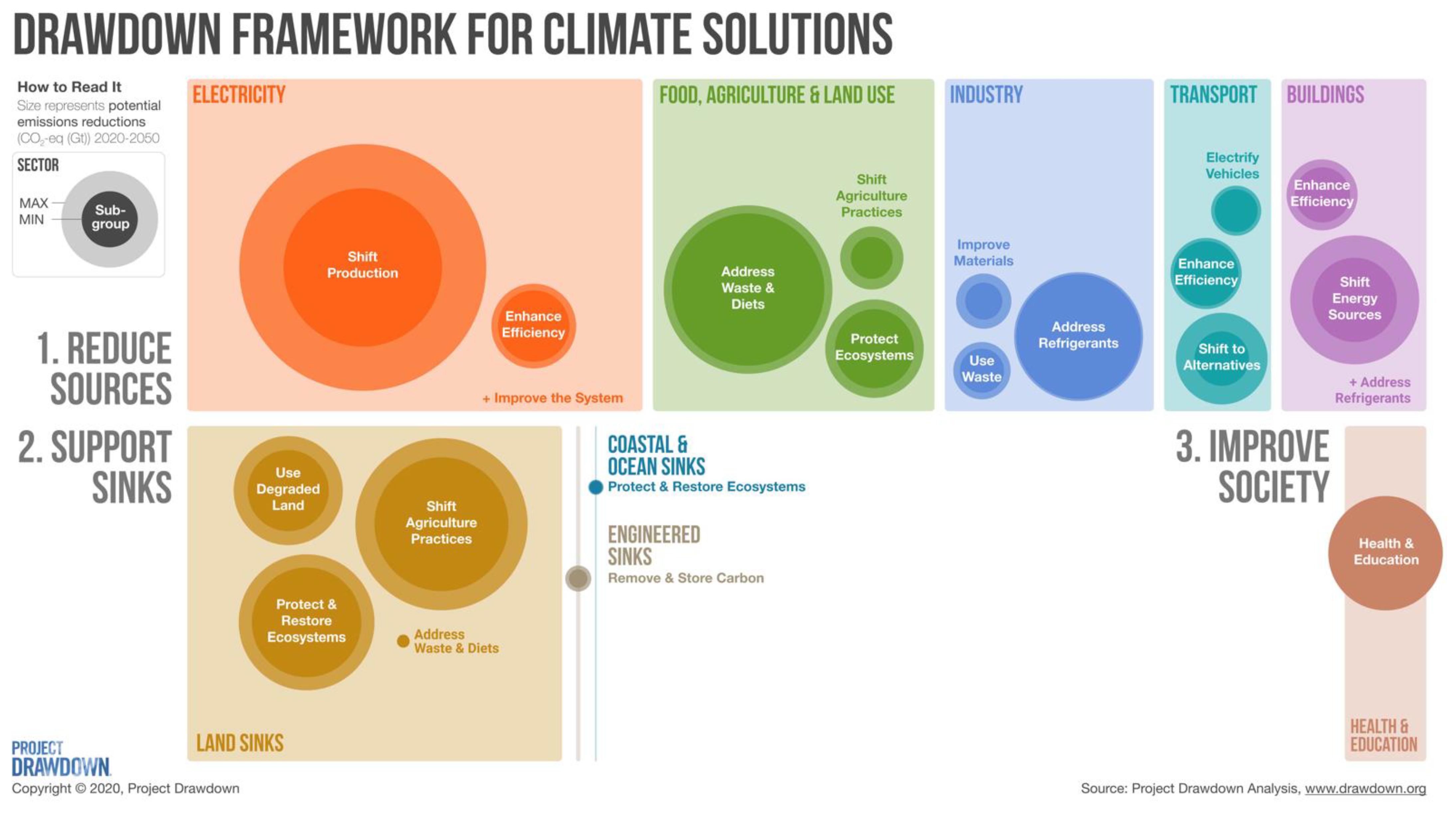
2. Climate Solutions Cut across Many Sectors
3. Improved Air Quality
4. Increased Physical Activity
5. Improved Nutrition and Food Security
6. Reduced Risk of Emerging Infectious Disease
7. Improved Sexual and Reproductive Health and Universal Education
8. Other Health Benefits of Climate Solutions
8.1. Reduced Exposure to Environmental Extremes
8.2. Improved Water Quality
8.3. Improved Mental Health
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masson-Delmotte, V.; Zhai, P.; Pirani, A.; Connors, S.L.; Péan, C.; Berger, S.; Caud, N.; Chen, Y.; Goldfarb, L.; Gomis, M.I.; et al. (Eds.) Intergovernmental Panel on Climate Change. Climate Change 2021: The Physical Science Basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK, 2021. [Google Scholar]
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Masson-Delmotte, V.; Zhai, P.; Pörtner, H.-O.; Roberts, D.; Skea, J.; Shukla, P.R.; Pirani, A.; Moufouma-Okia, W.; Péan, C.; Pidcock, R.; et al. (Eds.) Intergovernmental Panel on Climate Change. Summary for Policymakers. In Global Warming of 1.5°C. An IPCC Special Report on the Impacts of Global Warming of 1.5°C above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; World Meteorological Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Romanello, M.; McGushin, A.; Di Napoli, C.; Drummond, P.; Hughes, N.; Jamart, L.; Kennard, H.; Lampard, P.; Solano Rodriguez, B.; Arnell, N.; et al. The 2021 report of the Lancet Countdown on health and climate change: Code red for a healthy future. Lancet 2021, 398, 1619–1662. [Google Scholar] [CrossRef]
- Project Drawdown. The Drawdown Review: Climate Solutions for a New Decade; Project Drawdown: San Francisco, CA, USA, 2020. Available online: https://drawdown.org/drawdown-review (accessed on 16 December 2021).
- Haines, A.; Ebi, K. The Imperative for Climate Action to Protect Health. N. Engl. J. Med. 2019, 380, 263–273. [Google Scholar] [CrossRef]
- Patz, J.A.; Frumkin, H.; Holloway, T.; Vimont, D.J.; Haines, A. Climate Change: Challenges and Opportunities for Global Health. JAMA 2014, 312, 1565–1580. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Beagley, J.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; et al. The 2020 report of The Lancet Countdown on health and climate change: Responding to converging crises. Lancet 2020, 397, 129–170. [Google Scholar] [CrossRef]
- Quam, V.G.M.; Rocklöv, J.; Quam, M.B.M.; Lucas, R.A.I. Assessing Greenhouse Gas Emissions and Health Co-Benefits: A Structured Review of Lifestyle-Related Climate Change Mitigation Strategies. Int. J. Environ. Res. Public Health 2017, 14, 468. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.M.; Hess, J.J.; Balbus, J.M.; Buonocore, J.J.; Cleveland, D.A.; Grabow, M.L.; Neff, R.; Saari, R.K.; Tessum, C.W.; Wilkinson, P.; et al. Ancillary health effects of climate mitigation scenarios as drivers of policy uptake: A review of air quality, transportation and diet co-benefits modeling studies. Environ. Res. Lett. 2017, 12, 113001. [Google Scholar] [CrossRef]
- Haines, A.; McMichael, A.J.; Smith, K.R.; Roberts, I.; Woodcock, J.; Markandya, A.; Armstrong, B.G.; Campbell-Lendrum, D.; Dangour, A.D.; Davies, M.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Overview and implications for policy makers. Lancet 2009, 374, 2104–2114. [Google Scholar] [CrossRef]
- Gao, J.; Hou, H.; Zhai, Y.; Woodward, A.; Vardoulakis, S.; Kovats, S.; Wilkinson, P.; Li, L.; Song, X.; Xu, L.; et al. Greenhouse gas emissions reduction in different economic sectors: Mitigation measures, health co-benefits, knowledge gaps, and policy implications. Environ. Pollut. 2018, 240, 683–698. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.-M.; Liang, Q.-M.; Liu, L.-J.; Anadon, L.D. Co-benefits of greenhouse gas mitigation: A review and classification by type, mitigation sector, and geography. Environ. Res. Lett. 2017, 12, 123001. [Google Scholar] [CrossRef] [Green Version]
- Maibach, E.W.; Nisbet, M.; Baldwin, P.; Akerlof, K.; Diao, G. Reframing climate change as a public health issue: An exploratory study of public reactions. BMC Public Health 2010, 10, 299. [Google Scholar] [CrossRef] [Green Version]
- Stokes, L.C.; Warshaw, C. Renewable energy policy design and framing influence public support in the United States. Nat. Energy 2017, 2, 17107. [Google Scholar] [CrossRef]
- Amelung, D.; Fischer, H.; Herrmann, A.; Aall, C.; Louis, V.R.; Becher, H.; Wilkinson, P.; Sauerborn, R. Human health as a motivator for climate change mitigation: Results from T four European high-income countries. Glob. Environ. Chang. 2019, 57, 101918. [Google Scholar] [CrossRef]
- Maibach, E.W.; Sarfaty, M.; Mitchell, M.; Gould, R. Limiting global warming to 1.5 to 2.0 °C—A unique and necessary role for health professionals. PLoS Med. 2019, 16, e1002804. [Google Scholar] [CrossRef] [PubMed]
- Maibach, E.; Frumkin, H.; Ahdoot, S. Health Professionals and the Climate Crisis: Trusted Voices, Essential Roles. World Med. Health Policy 2021, 13, 137–145. [Google Scholar] [CrossRef]
- Maibach, E.; Miller, J.; Armstrong, F.; El Omrani, O.; Zhang, Y.; Philpott, N.; Atkinson, S.; Rudoph, L.; Karliner, J.; Wang, J.; et al. Health professionals, the Paris agreement, and the fierce urgency of now. J. Clim. Chang. Health 2021, 1, 100002. [Google Scholar] [CrossRef]
- Luong, K.T.; Kotcher, J.; Miller, J.; Campbell, E.; Epel, E.; Sarfaty, M.; Maibach, E. Prescription for healing the climate crisis: Insights on how to activate health professionals to advocate for climate and health solutions. J. Clim. Chang. Health 2021, 4, 100082. [Google Scholar] [CrossRef]
- Edenhofer, O.; Pichs-Madruga, R.; Sokona, Y.; Farahani, E.; Kadner, S.; Seyboth, K.; Adler, A.; Brunner, S.; Eickemeier, P.; Savolainen, J.; et al. (Eds.) Intergovernmental Panel on Climate Change. Climate Change 2014: Mitigation of Climate Change: Working Group III Contribution to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014. [Google Scholar]
- Institute for Health Metrics. GBD Compare. Available online: http://vizhub.healthdata.org/gbd-compare (accessed on 31 October 2021).
- Weagle, C.L.; Snider, G.; Li, C.; van Donkelaar, A.; Philip, S.; Bissonnette, P.; Burke, J.; Jackson, J.; Latimer, R.; Stone, E.; et al. Global Sources of Fine Particulate Matter: Interpretation of PM2.5 Chemical Composition Observed by SPARTAN using a Global Chemical Transport Model. Environ. Sci. Technol. 2018, 52, 11670–11681. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Lelieveld, J.; Klingmüller, K.; Pozzer, A.; Burnett, R.T.; Haines, A.; Ramanathan, V. Effects of fossil fuel and total anthropogenic emission removal on public health and climate. Proc. Natl. Acad. Sci. USA 2019, 116, 7192–7197. [Google Scholar] [CrossRef] [Green Version]
- Vohra, K.; Vodonos, A.; Schwartz, J.; Marais, E.A.; Sulprizio, M.P.; Mickley, L.J. Global mortality from outdoor fine particle pollution generated by fossil fuel combustion: Results from GEOS-Chem. Environ. Res. 2021, 195, 110754. [Google Scholar] [CrossRef] [PubMed]
- Millstein, D.; Wiser, R.; Bolinger, M.; Barbose, G. The climate and air-quality benefits of wind and solar power in the United States. Nat. Energy 2017, 2, 17134. [Google Scholar] [CrossRef]
- Anenberg, S.C.; Miller, J.; Henze, D.K.; Minjares, R.; Achakulwisut, P. The global burden of transportation tailpipe emissions on air pollution-related mortality in 2010 and 2015. Environ. Res. Lett. 2019, 14, 094012. [Google Scholar] [CrossRef]
- Shindell, D.T.; Lee, Y.; Faluvegi, G. Climate and health impacts of US emissions reductions consistent with 2 °C. Nat. Clim. Chang. 2016, 6, 503–507. [Google Scholar] [CrossRef]
- Liang, X.; Zhang, S.; Wu, Y.; Xing, J.; He, X.; Zhang, K.M.; Wang, S.; Hao, J. Air quality and health benefits from fleet electrification in China. Nat. Sustain. 2019, 2, 962–971. [Google Scholar] [CrossRef]
- Demetillo, M.A.G.; Harkins, C.; McDonald, B.C.; Chodrow, P.S.; Sun, K.; Pusede, S.E. Space-Based Observational Constraints on NO 2 Air Pollution Inequality From Diesel Traffic in Major US Cities. Geophys. Res. Lett. 2021, 48, 48. [Google Scholar] [CrossRef]
- Kerr, G.H.; Goldberg, D.L.; Anenberg, S.C. COVID-19 pandemic reveals persistent disparities in nitrogen dioxide pollution. Proc. Natl. Acad. Sci. USA 2021, 118, 2022409118. [Google Scholar] [CrossRef] [PubMed]
- Padoan, E.; Amato, F. Vehicle Non-Exhaust Emissions: Impact on Air Quality. In Non-Exhaust Emissions: An Urban Air Quality Problem for Public Health; Impact and Mitigation Measures; Amato, F., Ed.; Elsevier Inc.: London, UK, 2018; pp. 21–65. ISBN 978-0-12-811770-5. [Google Scholar]
- Victor, R.J.H.; Achten, P.A.J. Non-Exhaust PM Emissions from Battery Electric Vehicles. In Non-Exhaust Emissions: An Urban Air Quality Problem for Public Health; Impact and Mitigation Measures; Amato, F., Ed.; Elsevier Inc.: London, UK, 2018; pp. 261–287. ISBN 978-0-12-811770-5. [Google Scholar]
- Bisht, L.; Gupta, V.; Singh, A.; Gautam, A.S.; Gautam, S. Heavy metal concentration and its distribution analysis in urban road dust: A case study from most populated city of Indian state of Uttarakhand. Spat. Spatio-temporal Epidemiol. 2021, 40, 100470. [Google Scholar] [CrossRef]
- IEA; IRENA; UNSD; World Bank; WHO. Tracking SDG7: The Energy Progress Report 2021; World Bank: Washington, DC, USA, 2021. [Google Scholar]
- World Health Organization. Household Energy Database. Available online: https://www.who.int/data/gho/data/themes/air-pollution/who-household-energy-db (accessed on 31 October 2021).
- Anenberg, S.C.; Balakrishnan, K.; Jetter, J.; Masera, O.; Mehta, S.; Moss, J.; Ramanathan, V. Cleaner Cooking Solutions to Achieve Health, Climate, and Economic Cobenefits. Environ. Sci. Technol. 2013, 47, 3944–3952. [Google Scholar] [CrossRef]
- Van Gemert, F.; Air, F.; de Jong, C.; Kirenga, B.; Musinguzi, P.; Buteme, S.; Sooronbaev, T.; Tabyshova, A.; Emilov, B.; Mademilov, M.; et al. Effects and acceptability of implementing improved cookstoves and heaters to reduce household air pollution: A FRESH AIR study. Prim. Care Respir. Med. 2019, 29, 1–9. [Google Scholar] [CrossRef]
- Lacey, F.G.; Henze, D.K.; Lee, C.J.; van Donkelaar, A.; Martin, R.V. Transient climate and ambient health impacts due to national solid fuel cookstove emissions. Proc. Natl. Acad. Sci. USA 2017, 114, 1269–1274. [Google Scholar] [CrossRef] [Green Version]
- Thomas, E.G.; Wickramasinghe, K.; Mendis, S.; Roberts, N.; Foster, C. Improved stove interventions to reduce household air pollution in low and middle income countries: A descriptive systematic review. BMC Public Health 2015, 15, 41. [Google Scholar] [CrossRef] [Green Version]
- Quansah, R.; Semple, S.; Ochieng, C.A.; Juvekar, S.; Armah, F.A.; Luginaah, I.; Emina, J. Effectiveness of interventions to reduce household air pollution and/or improve health in homes using solid fuel in low-and-middle income countries: A systematic review and meta-analysis. Environ. Int. 2017, 103, 73–90. [Google Scholar] [CrossRef] [Green Version]
- Thakur, M.; Nuyts, P.A.W.; A Boudewijns, E.; Kim, J.F.; Faber, T.; Babu, G.R.; van Schayck, O.C.P.; Been, J.V. Impact of improved cookstoves on women’s and child health in low and middle income countries: A systematic review and meta-analysis. Thorax 2018, 73, 1026–1040. [Google Scholar] [CrossRef] [PubMed]
- Norris, C.; Goldberg, M.S.; Marshall, J.D.; Valois, M.-F.; Pradeep, T.; Narayanswamy, M.; Jain, G.; Sethuraman, K.; Baumgartner, J. A panel study of the acute effects of personal exposure to household air pollution on ambulatory blood pressure in rural Indian women. Environ. Res. 2016, 147, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Onakomaiya, D.; Gyamfi, J.; Iwelunmor, J.; Opeyemi, J.; Oluwasanmi, M.; Obiezu-Umeh, C.; Dalton, M.; Nwaozuru, U.; Ojo, T.; Vieira, D.; et al. Implementation of clean cookstove interventions and its effects on blood pressure in low-income and middle-income countries: Systematic review. BMJ Open 2019, 9, e026517. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Balmes, J.R.; de Matteis, S.; Hoffman, B.; Kim, W.J.; Perez-Padilla, R.; Rice, M.; Sood, A.; Vanker, A.; Wuebbles, D.J. Health Benefits of Air Pollution Reduction. Ann. Am. Thorac. Soc. 2019, 16, 1478–1487. [Google Scholar] [CrossRef]
- Ho, E.W.; Strohmeier-Breuning, S.; Rossanese, M.; Charron, D.; Pennise, D.; Graham, J.P. Diverse Health, Gender and Economic Impacts from Domestic Transport of Water and Solid Fuel: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 10355. [Google Scholar] [CrossRef]
- Lelieveld, J.; Pozzer, A.; Pöschl, U.; Fnais, M.; Haines, A.; Münzel, T. Loss of life expectancy from air pollution compared to other risk factors: A worldwide perspective. Cardiovasc. Res. 2020, 116, 1910–1917. [Google Scholar] [CrossRef] [PubMed]
- Tessum, C.W.; Apte, J.S.; Goodkind, A.L.; Muller, N.Z.; Mullins, K.A.; Paolella, D.A.; Polasky, S.; Springer, N.P.; Thakrar, S.K.; Marshall, J.D.; et al. Inequity in consumption of goods and services adds to racial–ethnic disparities in air pollution exposure. Proc. Natl. Acad. Sci. USA 2019, 116, 6001–6006. [Google Scholar] [CrossRef] [Green Version]
- Tessum, C.W.; Paolella, D.A.; Chambliss, S.E.; Apte, J.S.; Hill, J.D.; Marshall, J.D. PM 2.5 polluters disproportionately and systemically affect people of color in the United States. Sci. Adv. 2021, 7, eabf4491. [Google Scholar] [CrossRef]
- Wang, L.; Zhong, B.; Vardoulakis, S.; Zhang, F.; Pilot, E.; Li, Y.; Yang, L.; Wang, W.; Krafft, T. Air Quality Strategies on Public Health and Health Equity in Europe—A Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, M.D.; Kinney, P.L.; Southerland, V.; Arno, C.A.; Crawford, K.; van Donkelaar, A.; Hammer, M.; Martin, R.V.; Anenberg, S.C. Estimating intra-urban inequities in PM2.5-attributable health impacts: A case study for Washington, DC. GeoHealth 2021, 5, e2021GH000431. [Google Scholar] [CrossRef] [PubMed]
- Cartier, Y.; Benmarhnia, T.; Brousselle, A. Tool for assessing health and equity impacts of interventions modifying air quality in urban environments. Eval. Program Plan. 2015, 53, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.P.; Marshall, J.D. Impact, efficiency, inequality, and injustice of urban air pollution: Variability by emission location. Environ. Res. Lett. 2018, 13, 024002. [Google Scholar] [CrossRef]
- Heyer, J.; Palm, M.; Niemeier, D. Are we keeping up? Accessibility, equity and air quality in regional planning. J. Transp. Geogr. 2020, 89, 102891. [Google Scholar] [CrossRef]
- Hajat, A.; Hsia, C.; O’Neill, M.S. Socioeconomic Disparities and Air Pollution Exposure: A Global Review. Curr. Environ. Health Rep. 2015, 2, 440–450. [Google Scholar] [CrossRef] [Green Version]
- Younger, M.; Morrow-Almeida, H.R.; Vindigni, S.M.; Dannenberg, A.L. The Built Environment, Climate Change, and Health. Am. J. Prev. Med. 2008, 35, 517–526. [Google Scholar] [CrossRef]
- Lowe, M.; Boulange, C.; Giles-Corti, B. Urban design and health: Progress to date and future challenges: Urban Design and Health. Health Promot. J. Austr. 2014, 25, 14–18. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef]
- Stevenson, M.; Thompson, J.; de Sá, T.H.; Ewing, R.; Mohan, D.; McClure, R.; Roberts, I.; Tiwari, G.; Giles-Corti, B.; Sun, X.; et al. Land use, transport, and population health: Estimating the health benefits of compact cities. Lancet 2016, 388, 2925–2935. [Google Scholar] [CrossRef] [Green Version]
- Strain, T.; Brage, S.; Sharp, S.J.; Richards, J.; Tainio, M.; Ding, D.; Benichou, J.; Kelly, P. Use of the prevented fraction for the population to determine deaths averted by existing prevalence of physical activity: A descriptive study. Lancet Glob. Health 2020, 8, e920–e930. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Panis, L.I.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Pucher, J.; Buehler, R.; Bassett, D.R.; Dannenberg, A.L. Walking and Cycling to Health: A Comparative Analysis of City, State, and International Data. Am. J. Public Health 2010, 100, 1986–1992. [Google Scholar] [CrossRef]
- Tehrani, S.O.; Wu, S.J.; Roberts, J.D. The Color of Health: Residential Segregation, Light Rail Transit Developments, and Gentrification in the United States. Int. J. Environ. Res. Public Health 2019, 16, 3683. [Google Scholar] [CrossRef] [Green Version]
- Myers, S.; Frumkin, H. (Eds.) Planetary Health: Protecting Nature to Protect Ourselves; Island Press: Washington, DC, USA, 2020. [Google Scholar]
- Gustavsson, J. (Ed.) Food and Agricultural Organization. Global Food Losses and Food Waste: Extent, Causes and Prevention; Food and Agriculture Organization of the United Nations: Rome, Italy, 2011. [Google Scholar]
- Springmann, M.; Godfray, H.C.J.; Rayner, M.; Scarborough, P. Analysis and valuation of the health and climate change cobenefits of dietary change. Proc. Natl. Acad. Sci. USA 2016, 113, 4146–4151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Tubiello, F.N.; Rosenzweig, C.; Conchedda, G.; Karl, K.; Gütschow, J.; Xueyao, P.; Obli-Laryea, G.; Wanner, N.; Qiu, S.Y.; de Barros, J.; et al. Greenhouse gas emissions from food systems: Building the evidence base. Environ. Res. Lett. 2021, 16, 065007. [Google Scholar] [CrossRef]
- Adesogan, A.T.; Havelaar, A.H.; McKune, S.L.; Eilittä, M.; Dahl, G.E. Animal source foods: Sustainability problem or malnutrition and sustainability solution? Perspective matters. Glob. Food Secur. 2020, 25, 100325. [Google Scholar] [CrossRef]
- Dasgupta, P. The Economics of Biodiversity: The Dasgupta Review; HM Treasury: London, UK, 2021. [Google Scholar]
- Brondízio, E.S.; Settele, J.; Díaz, S.; Ngo, H.T. (Eds.) Global Assessment Report of the Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services; Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services: Bonn, Germany, 2019. [Google Scholar]
- Naidoo, R.; Gerkey, D.; Hole, D.; Pfaff, A.; Ellis, A.M.; Golden, C.D.; Herrera, D.; Johnson, K.; Mulligan, M.; Ricketts, T.H.; et al. Evaluating the impacts of protected areas on human well-being across the developing world. Sci. Adv. 2019, 5, eaav3006. [Google Scholar] [CrossRef] [Green Version]
- Rosset, P.M.; Martínez-Torres, M.E. Rural Social Movements and Agroecology: Context, Theory, and Process. Ecol. Soc. 2012, 17, 17. [Google Scholar] [CrossRef]
- Plowright, R.K.; Reaser, J.K.; Locke, H.; Woodley, S.J.; Patz, J.A.; Becker, D.J.; Oppler, G.; Hudson, P.J.; Tabor, G.M. Land use-induced spillover: A call to action to safeguard environmental, animal, and human health. Lancet Planet. Health 2021, 5, e237–e245. [Google Scholar] [CrossRef]
- Johns Hopkins University. Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 5 December 2021).
- Center for Disease Control and Prevention. History of Ebola Virus Disease (EVD) Outbreaks. Available online: https://www.cdc.gov/vhf/ebola/history/chronology.html (accessed on 31 October 2021).
- Rulli, M.C.; Santini, M.; Hayman, D.T.S.; D’Odorico, P. The nexus between forest fragmentation in Africa and Ebola virus disease outbreaks. Sci. Rep. 2017, 7, 41613. [Google Scholar] [CrossRef] [Green Version]
- Olivero, J.; Fa, J.E.; Real, R.; Márquez, A.L.; Farfán, M.A.; Vargas, J.M.; Gaveau, D.; Salim, M.A.; Park, D.; Suter, J.; et al. Recent loss of closed forests is associated with Ebola virus disease outbreaks. Sci. Rep. 2017, 7, 14291. [Google Scholar] [CrossRef] [Green Version]
- Vittor, A.Y.; Pan, W.; Gilman, R.H.; Tielsch, J.; Glass, G.; Shields, T.; Sánchez-Lozano, W.; Pinedo, V.V.; Salas-Cobos, E.; Flores, S.; et al. Linking deforestation to malaria in the Amazon: Characterization of the breeding habitat of the principal malaria vector, Anopheles darlingi. Am. J. Trop. Med. Hyg. 2009, 81, 5–12. [Google Scholar]
- Olson, S.H.; Gangnon, R.; Elguero, E.; Durieux, L.; Guégan, J.-F.; Foley, J.A.; Patz, J.A. Links between Climate, Malaria, and Wetlands in the Amazon Basin. Emerg. Infect. Dis. 2009, 15, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Vittor, A.Y.; Gilman, R.H.; Tielsch, J.; Glass, G.; Shields, T.; Lozano, W.S.; Pinedo-Cancino, V.; Patz, J.A. The effect of deforestation on the human-biting rate of anopheles darlingi, the primary vector of falciparum malaria in the peruvian amazon. Am. J. Trop. Med. Hyg. 2006, 74, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, T. Ecosystems and human health: The local benefits of forest cover in Indonesia. J. Environ. Econ. Manag. 2019, 98, 102271. [Google Scholar] [CrossRef] [Green Version]
- Lindblade, K.A.; Walker, E.D.; Onapa, A.W.; Katungu, J.; Wilson, M.L. Land use change alters malaria transmission parameters by modifying temperature in a highland area of Uganda. Trop. Med. Int. Health 2000, 5, 263–274. [Google Scholar] [CrossRef]
- O’Neill, B.C.; Dalton, M.; Fuchs, R.; Jiang, L.; Pachauri, S.; Zigova, K. Global demographic trends and future carbon emissions. Proc. Natl. Acad. Sci. USA 2010, 107, 17521–17526. [Google Scholar] [CrossRef] [Green Version]
- Dodson, J.C.; Dérer, P.; Cafaro, P.; Götmark, F. Population growth and climate change: Addressing the overlooked threat multiplier. Sci. Total. Environ. 2020, 748, 141346. [Google Scholar] [CrossRef]
- Liu, D.H.; Raftery, A.E. How Do Education and Family Planning Accelerate Fertility Decline? Popul. Dev. Rev. 2020, 46, 409–441. [Google Scholar] [CrossRef] [PubMed]
- Psaki, S.R.; Chuang, E.K.; Melnikas, A.J.; Wilson, D.B.; Mensch, B.S. Causal effects of education on sexual and reproductive health in low and middle-income countries: A systematic review and meta-analysis. SSM—Popul. Health 2019, 8, 100386. [Google Scholar] [CrossRef] [PubMed]
- Starrs, A.M.; Ezeh, A.C.; Barker, G.; Basu, A.; Bertrand, J.T.; Blum, R.; Coll-Seck, A.M.; Grover, A.; Laski, L.; Roa, M.; et al. Accelerate progress—Sexual and reproductive health and rights for all: Report of the Guttmacher–Lancet Commission. Lancet 2018, 391, 2642–2692. [Google Scholar] [CrossRef]
- Hardee, K.; Patterson, K.P.; Schenck-Fontaine, A.; Hess, S.; Leisher, C.; Mutunga, C.; Margoluis, C.; Honzak, C. Family planning and resilience: Associations found in a Population, Health, and Environment (PHE) project in Western Tanzania. Popul. Environ. 2018, 40, 204–238. [Google Scholar] [CrossRef] [Green Version]
- Frischmann, C.J.; Mehra, M.; Allard, R.; Bayuk, K.; Gouveia, J.P.; Gorman, M.R. Drawdown’s “System of Solutions” Helps to Achieve the SDGs. In Partnerships for the Goals; Leal Filho, W., Azul, A.M., Brandli, L., Lange Salvia, A., Wall, T., Eds.; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar]
- Gakidou, E.; Cowling, K.; Lozano, R.; Murray, C.J. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: A systematic analysis. Lancet 2010, 376, 959–974. [Google Scholar] [CrossRef]
- Viner, R.M.; Hargreaves, D.S.; Ward, J.; Bonell, C.; Mokdad, A.H.; Patton, G. The health benefits of secondary education in adolescents and young adults: An international analysis in 186 low-, middle- and high-income countries from 1990 to 2013. SSM—Popul. Health 2017, 3, 162–171. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, B.C.; Jiang, L.; Kc, S.; Fuchs, R.; Pachauri, S.; Laidlaw, E.K.; Zhang, T.; Zhou, W.; Ren, X. The effect of education on determinants of climate change risks. Nat. Sustain. 2020, 3, 520–528. [Google Scholar] [CrossRef]
- Sims, K. Education, Girls’ Education and Climate Change. K4D Emerging Issues Report 29; Institute of Development Studies: Brighton, UK, 2021. [Google Scholar] [CrossRef]
- Striessnig, E.; Lutz, W.; Patt, A.G. Effects of Educational Attainment on Climate Risk Vulnerability. Ecol. Soc. 2013, 18, 18. [Google Scholar] [CrossRef] [Green Version]
- Kwauk, C.; Casey, O. A Green Learning Agenda: Approaches to Quality Education for Climate Action; The Brookings Institution: Washington, DC, USA, 2021. [Google Scholar]
- Fry, L.; Lei, P. A Greener, Fairer Future: Why Leaders Need to Invest in Climate and Girls’ Education; Issa, M., Thomas, T., Eds.; Malala Fund: Washington, DC, USA, 2021. [Google Scholar]
- Van Coppenolle, R.; Temmerman, S. Identifying global hotspots where coastal wetland conservation can contribute to nature-based mitigation of coastal flood risks. Glob. Planet. Change 2020, 187, 103125. [Google Scholar] [CrossRef]
- Quaranta, E.; Dorati, C.; Pistocchi, A. Water, Energy and Climate Benefits of Urban Greening throughout Europe under Dif-ferent Climatic Scenarios. Sci. Rep. 2021, 11, 12163. [Google Scholar] [CrossRef]
- Lamb, J.B.; van de Water, J.A.J.M.; Bourne, D.G.; Altier, C.; Hein, M.Y.; Fiorenza, E.A.; Abu, N.; Jompa, J.; Harvell, C.D. Seagrass ecosystems reduce exposure to bacterial pathogens of humans, fishes, and invertebrates. Science 2017, 355, 731–733. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [Green Version]
- Myers, S.S. Planetary health: Protecting human health on a rapidly changing planet. Lancet 2017, 390, 2860–2868. [Google Scholar] [CrossRef]
- Gould, R.; Harp, B.D.; Nackerman, C.; Maibach, E. Developing equitable health and climate solutions: Insights from the field. Environ. Res. Lett. 2021, 16, 011002. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Health Theme | Health Benefits |
|---|---|
| Improved air quality | Improved cardiovascular and respiratory health (e.g., lower incidence of heart disease, stroke, lung cancer, diabetes, chronic obstructive pulmonary disease, pneumonia) |
| Increased physical activity | Reduced cardiovascular disease, diabetes, and impaired mental health; lowered risk of obesity-related illness |
| Improved nutrition and food security | Improved cardiovascular health (e.g., lower incidence of heart disease, stroke, and diabetes) |
| Reduced risk of emerging infectious disease | Reduced risk of exposure to zoonotic and vector-borne disease (e.g., Hendra virus, Ebola virus, and malaria) |
| Reduced exposure to environmental extremes | Reduced exposure to natural hazards (e.g., coastal and inland flooding, extreme heat, storm surge from cyclone activity) |
| Improved water quality | Reduced risk of water-borne disease (e.g., diarrheal disease) and toxics exposure |
| Improved mental health | Reduced prevalence of stress, depression, and anxiety |
| Improved sexual and reproductive health | Gender equality; reduced maternal, newborn, child, and adolescent mortality; reduced vulnerability to environmental stressors and climate-related extreme events |
| Universal education | Improved health, empowerment, climate adaptation, and resilience; reduced risk of HIV infection |
| Area | Sector and Subgroup | Climate Solutions | Health Themes |
|---|---|---|---|
| Reduce Sources | Electricity | ||
| Shift production | Distributed solar photovoltaics; utility-scale solar photovoltaics; onshore wind turbines; offshore wind turbines; geothermal power; biomass power; nuclear power | Improved air quality | |
| Enhance efficiency | Smart thermostats; building automation systems; LED lighting; insulation; green and cool roofs; high-efficiency heat pumps; solar hot water; building retrofitting | Improved air quality | |
| Transportation | |||
| Shift to alternatives | Walkable cities; bicycle infrastructure; electric bicycles; carpooling; public transit; high-speed rail | Improved air quality; increased physical activity | |
| Enhance efficiency | Hybrid cars; efficient trucks; efficient aviation; efficient ocean shipping | Improved air quality | |
| Electrify vehicles | Electric cars; electric trains | Improved air quality | |
| Buildings | |||
| Enhance efficiency | See: Electricity | ||
| Shift energy sources | Biogas for cooking; improved clean cookstoves | Improved air quality | |
| Food, agriculture, and land use | |||
| Address diets and waste | Plant-rich diets; reduced food waste | Improved nutrition and food security | |
| Protect ecosystems | See: Land sinks | ||
| Shift agriculture practices | Nutrient management; farm irrigation efficiency | Improved water quality | |
| Support Sinks | Land sinks | ||
| Address waste and diets | Plant-rich diets; reduced food waste | Improved nutrition and food security | |
| Protect and restore ecosystems | Forest protection; indigenous peoples’ land tenure; temperate forest restoration; tropical forest restoration; grassland protection; peatland protection and rewetting | Reduced risk of emerging infectious disease; reduced exposure to environmental extremes; improved water quality; improved mental health | |
| Coastal and ocean sinks | |||
| Protect and restore ecosystems | Coastal wetland protection; coastal wetland restoration | Reduced exposure to environmental extremes | |
| Improve Society | Health and education | ||
| Health and education | Voluntary, rights-based family planning; universal, high-quality education | Improved sexual and reproductive health; universal education |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mailloux, N.A.; Henegan, C.P.; Lsoto, D.; Patterson, K.P.; West, P.C.; Foley, J.A.; Patz, J.A. Climate Solutions Double as Health Interventions. Int. J. Environ. Res. Public Health 2021, 18, 13339. https://doi.org/10.3390/ijerph182413339
Mailloux NA, Henegan CP, Lsoto D, Patterson KP, West PC, Foley JA, Patz JA. Climate Solutions Double as Health Interventions. International Journal of Environmental Research and Public Health. 2021; 18(24):13339. https://doi.org/10.3390/ijerph182413339
Chicago/Turabian StyleMailloux, Nicholas A., Colleen P. Henegan, Dorothy Lsoto, Kristen P. Patterson, Paul C. West, Jonathan A. Foley, and Jonathan A. Patz. 2021. "Climate Solutions Double as Health Interventions" International Journal of Environmental Research and Public Health 18, no. 24: 13339. https://doi.org/10.3390/ijerph182413339